ELSEVIER Lung Cancer 16 (1996) 95-100 LUNG CANCER Endobronchial extramedullary plasmacytoma. Report of one case A. Terzi”**, G. Furlan”, M. Zannonib, A. Adovasio”, A. Gorla” “Divisione di Chirurgia Toracica, Ospeahle Civile Maggiore Azienda Ospedaliera Verona. P. le Stefani 1 37126 Verona, Italy bServizio di Anatomia Patologica, Ospedale Civile Maggiore, Azienda Ospedaliera Verona, Verona, Italy ‘Divisione di Medicina, Ospedale di Poggiorusco, Mantova, Italy Received 24 June 1996; revised 7 October 1996; accepted 9 October 1996 Abstract A patient underwent a subtotal resection of the tracheobronchial carina for an obstructing endobronchial lesion. Preoperative biopsies of the lesion were not diagnostic. After resection, the histological examination of the specimen removed demonstrated an extramedullary plasmacytoma infiltrating the bronchial wall. Immunohistochemical studies showed mono- clonality for kappa light chains. The postoperative course was uneventful and the screening for multiple myeloma was negative. No adjuvant treatment was given and the patient is currently alive and free of disease 63 months after the resection. Primary endobronchial plasmacytoma is a very rare disease; it is unclear which is the best treatment for endo- bronchial plasmacytoma. However. complete surgical resection has allowed a long-term survival, free of disease. Copyright 0 1996 Elsevier Science Ireland Ltd. Keywords: Plasmacytoma: Extramedullary plasmacytoma; Endobronchial plasmacytoma * Corresponding author. Tel: + 39-45-8072312; Fax: + 39-45-8072046 0169-5002/96/$15.00 Copyright 0 1996 Elsevier Science Ireland Ltd. All rights reserved PIISO169-5002(96)00616-2
Transcript
ELSEVIER Lung Cancer 16 (1996) 95-100
LUNG CANCER
Endobronchial extramedullary plasmacytoma. Report of one case
A. Terzi”**, G. Furlan”, M. Zannonib, A. Adovasio”, A. Gorla” “Divisione di Chirurgia Toracica, Ospeahle Civile Maggiore Azienda Ospedaliera Verona.
P. le Stefani 1 37126 Verona, Italy bServizio di Anatomia Patologica, Ospedale Civile Maggiore, Azienda Ospedaliera Verona,
Verona, Italy ‘Divisione di Medicina, Ospedale di Poggiorusco, Mantova, Italy
Received 24 June 1996; revised 7 October 1996; accepted 9 October 1996
Abstract
A patient underwent a subtotal resection of the tracheobronchial carina for an obstructing endobronchial lesion. Preoperative biopsies of the lesion were not diagnostic. After resection, the histological examination of the specimen removed demonstrated an extramedullary plasmacytoma infiltrating the bronchial wall. Immunohistochemical studies showed mono- clonality for kappa light chains. The postoperative course was uneventful and the screening for multiple myeloma was negative. No adjuvant treatment was given and the patient is currently alive and free of disease 63 months after the resection. Primary endobronchial plasmacytoma is a very rare disease; it is unclear which is the best treatment for endo- bronchial plasmacytoma. However. complete surgical resection has allowed a long-term survival, free of disease. Copyright 0 1996 Elsevier Science Ireland Ltd.
0169-5002/96/$15.00 Copyright 0 1996 Elsevier Science Ireland Ltd. All rights reserved PIISO169-5002(96)00616-2
96 A. Terri et al. /Lung Cancer 16 (1996) 95-100
1. Introduction
Extramedullary plasmacytomas are plasma cell neoplasms usually located in the nasopharynx and upper respiratory tract; their diagnosis is made by histological examination of a biopsy specimen in the absence of systemic signs and symptoms of multiple myeloma and with a bone marrow specimen showing less then 10% plasma cells. Non-metastatic pulmonary plasmacytoma is rare and endobronchial primary plasmacytoma is even rarer as only three cases have been reported [1,3]. The present case illustrates a primary plasmacytoma of the tracheobronchial carina treated by subtotal carinal resection.
2. Case report
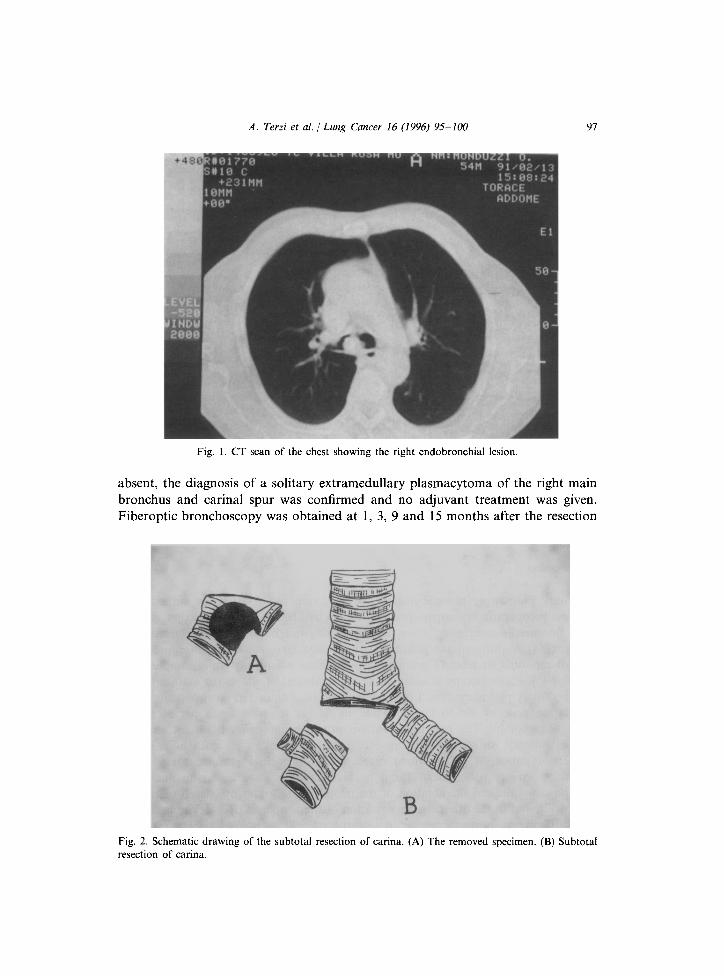
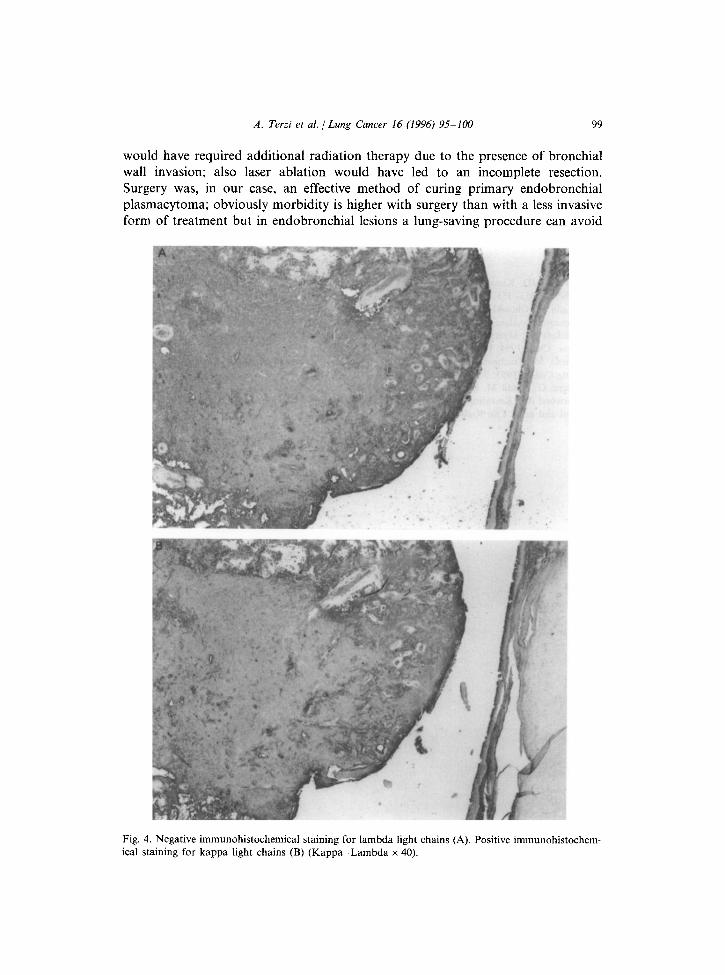
A 65-year-old man complaining of mild dyspnoea on exertion and a non-produc- tive cough came under observation. His symptoms had begun about 2 months before; he had no smoking history. On physical examination a reduction of vesicular murmur was appreciated on the right side of the chest. Laboratory studies (urine and blood) were all in the normal range, chest X-ray was normal, a bronchoscopy showed the presence of a reddish mass subtotally obstructing the right main bronchus, originating on the medial part of the right main bronchus and involving the carinal spur; exploration of the right bronchial tree was not possible. Multiple biopsies of the lesion were taken and sent for histological examination. A CT scan of the chest showed an endobronchial lesion at the level of tracheo- bronchial carina approximately 2 cm in diameter and no mediastinal adenopathy (Fig. 1); a CT scan of abdomen and brain was negative. As biopsy specimens were not diagnostic, the patient eventually underwent surgery. The patient was intubated with a double lumen endotracheal tube and the chest was entered by a standard right posterolateral thoracotomy; carinal and right paratracheal nodes were re- moved and sent for histopathological examination, then a subtotal resection of the trachea-bronchial carina was performed (Fig. 2); a neocarina was then constructed by first anastomosing the medial part of the right and left main bronchus and then anastomosing them to the trachea [4]; high frequency jet ventilation was used during carinal resection and reconstruction. The postoperative course was unevent- ful, the endoscopic control of the anastomosis showed a good healing and the patient was discharged 14 days after the operation. Histologic review demonstrated a neoplasm composed of large monomorphic oval cells with eccentric nuclei (Fig. 3) invading the bronchial wall; the margins of resection were clear of tumor. Immuno- histochemical stainings were negative for keratin, leucocyte common antigen, calcitonin, cromogranine and sinaptophysine; the tumor cells showed monoclonal- ity for kappa light chains (Fig. 4), therefore the findings were consistent with plasmacytoma. After the histological diagnosis a screening for multiple myeloma, including serum and urine electrophoresis, a bone marrow analysis and bone X-rays were obtained. As neither hyperglobulinemia nor globulin peak on serum or urine were detected and bone marrow plasma cells infiltration or area of osteolysis were
A. Terzi et al. / Lung Cancer 16 (1996) 95-100 91
Fig. 1. CT scan of the chest showing the right endobronchial lesion.
absent, the diagnosis of a solitary extramedullary plasmacytoma of the right main bronchus and carinal spur was confirmed and no adjuvant treatment was given. Fiberoptic bronchoscopy was obtained at 1, 3, 9 and 15 months after the resection
Fig. 2. Schematic drawing of the subtotal resection of carina. (A) The removed specimen. (B) Subtotal resection of carina.
98 A. Terzi et al. / Lung Cancer 16 (1996) 95- 100
Fig. 3. Endobronchial neoplasm composed of monomorphic large oval cells with eccentric nuclei and unusually prominent nucleoli (Ciiemsa x 400).
and then yearly; serum electrophoresis obtained yearly showed no abnormality (no M-component) and the patient is alive free of disease 63 months later.
3. Discussion
Primary pulmonary plasmacytomas are very rare tumors that are difficult to diagnose preoperatively; biopsy specimens taken by fiberoptic bronchoscopy as well as by fine needle aspiration, when indicated, may not be diagnostic. Uncertainty often exists to differentiate pulmonary plasmacytoma, plasma cell granuloma, pseudolymphoma or reactive granulomatous lesions when only small samples are available [5]. Radiotherapy is accepted as the treatment of choice for extrathoracic extramedullary plasmacytoma. Local control can be obtained in most patients with a radiation dose of 40-50 Gy [3] while surgery is reserved for a persistent or recurrent tumor [6]. The best treatment for primary pulmonary plasmacytoma is, on the contrary, still unclear because of insufficient follow-up data in a small number of patients [5]. The three cases of endobronchial plasmacytoma were treated by surgery (one case) [l] and by bronchoscopy (two cases); in one case bronchoscopy allowed the ablation of the neoplasm, followed by chemo-radiation therapy [2], and in the other the vaporization of the neoplasm by Nd-Yag laser [3]; none of them has shown recurrence in a short-term follow-up. We have aggressively treated our patient and he is alive without recurrence after 63 months; furthermore, loss of pulmonary parenchyma has been avoided. In our case endoscopic resection
A. Terzi et al. / Lung Cancer 16 (1996) 95-100 99
would have required additional radiation therapy due to the presence of bronchial wall invasion; also laser ablation would have led to an incomplete resection. Surgery was, in our case, an effective method of curing primary endobronchial plasmacytoma; obviously morbidity is higher with surgery than with a less invasive form of treatment but in endobronchial lesions a lung-saving procedure can avoid
Fig. 4. Negative immunohistochemical staining for lambda light chains (A). Positive immunohistochem- ical staining for kappa light chains (B) (Kappa-Lambda x 40).
100 A. Terzi et al. / Lung Cancer 16 (1996) 9% 100
loss of pulmonary parenchyma, as in our case. In this particular location, contrary to other locations, consideration should be given to the fact that carinal resection after radiotherapy, should radiotherapy fail to control the disease, is at great risk for a potentially fatal complication like bronchopleural fistula.
References
[I] Kennedy JD, Kneafsey DV. Two cases of plasmacytoma of the lower respiratory tract. Thorax 1959; 14: 353-355.
[2] Okada S, Ohtsuki H, Midorikawa 0, Hoshimoto K. Bronchial plasmacytoma identified by immunoperoxidase technique on paraffin embedded section. Acta Path01 Jpn 1982; 32: 1499155.
[3] Brackett LE, Myers JR, Sherman CB. Laser treatment of endobronchial extramedullary plasmacy- toma. Chest 1994; 106: 1276-1277.
[4] Maeda M. Tracheobronchial resection for tumor:classification and related biological problems Lung Cancer 1993; 9: 191-201.
[5] Joseph G, Pandit M, Korfhage L. Primary pulmonary plasmacytoma. Cancer 1993; 71: 721-724. [6] Harwood AR, Knowling MA, Bergsagel DE. Radiotherapy of extramedullary plasmacytoma of the