46
Prevenire lo scompenso e le sue recidive La terapia non farmacologica Sessione II - Prevenzione, Terapia, Riabilitazione dello Scompenso Cardiaco

Prevenire lo scompenso e le sue recidive
La terapia non
farmacologica
Sessione II - Prevenzione, Terapia,
Riabilitazione dello Scompenso
Cardiaco

Prevenire lo scompenso e le sue recidive
La terapia non farmacologica dello scompenso cardiaco
cronico consiste nell’attuazione di misure strumentali
invasive e/o propriamente chirurgiche per il trattamento dei
casi refrattari alla terapia medica condotta in modo ottimale e
appropriato
Le procedure oggi attuate sono:
•Terapia elettrica (ICD, CRT-P, CRT-D)
•Ultrafiltrazione
•Terapia invasiva percutanea
•Terapia chirurgica
Terapia non farmacologica; Classificazione:

Prevenire lo scompenso e le sue recidive
Terapia Elettrica
Terapia non farmacologica;
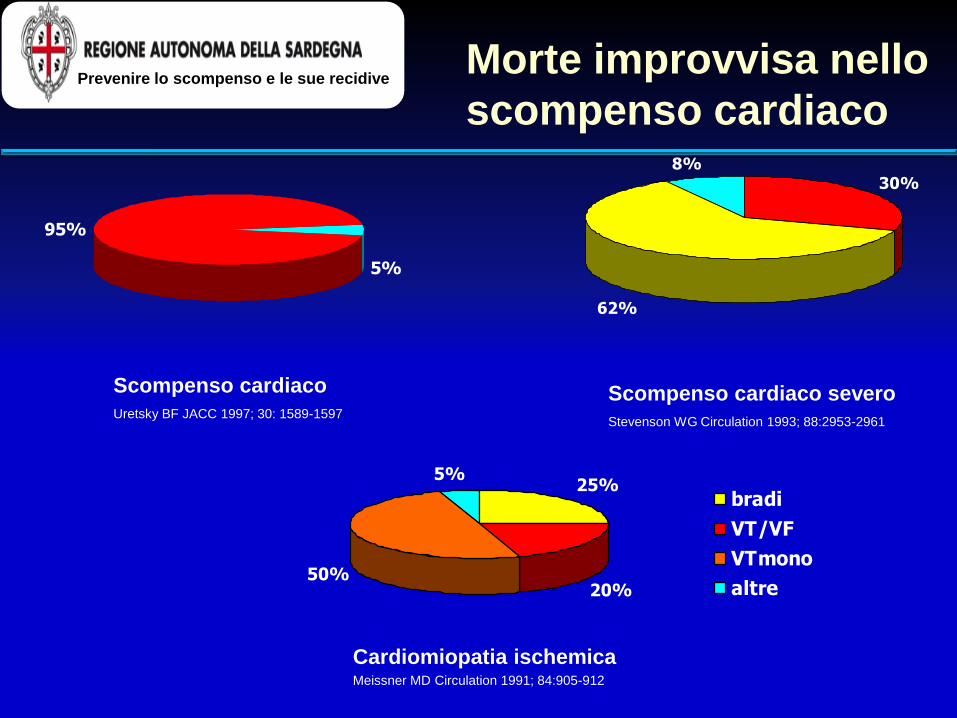
Morte improvvisa nello
scompenso cardiaco
Cardiomiopatia ischemica Meissner MD Circulation 1991; 84:905-912
95%
5%
Scompenso cardiaco severo
Stevenson WG Circulation 1993; 88:2953-2961
Scompenso cardiaco
Uretsky BF JACC 1997; 30: 1589-1597
30%
62%
8%
25%
20%50%
5%
bradi
VT/VF
VTmono
altre
Prevenire lo scompenso e le sue recidive
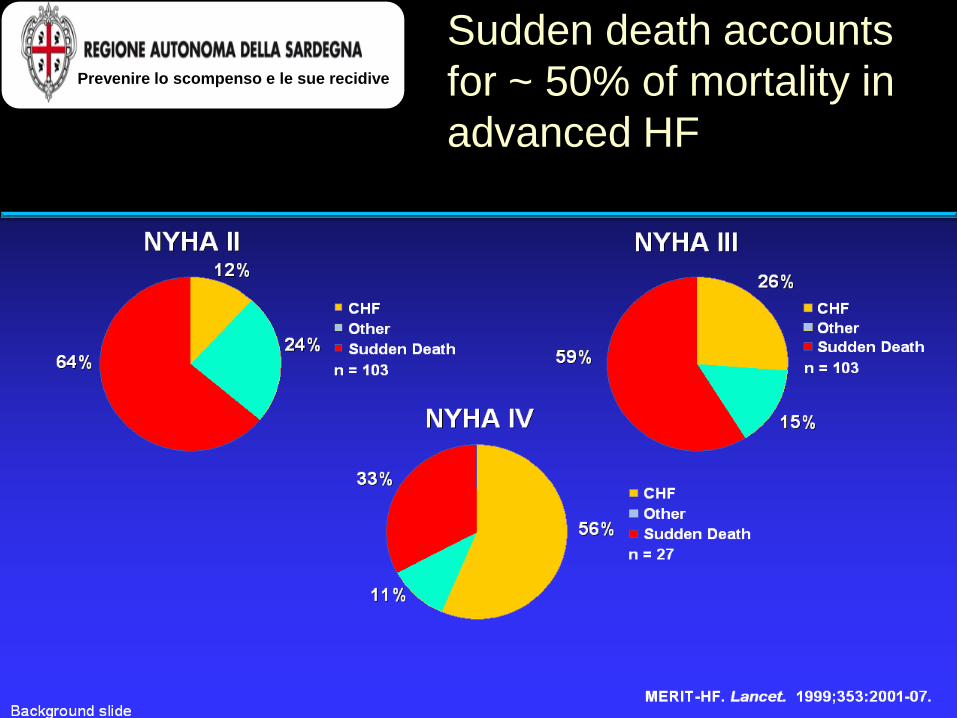
Sudden death accounts
for ~ 50% of mortality in
advanced HF
Prevenire lo scompenso e le sue recidive

0
5
10
15
20
25
30
35
40
NYHA I II III IV
% 1
ye
ar
mo
rta
lity
morte improvvisa mortalità totale
SOLVD-Pre
DIG 1996
SOLVD-Treat
V-HeFT II
ELITE 1997
CARVEDILOL
UCLA
VESNARINONE
CONSENSUS
Stevenson WG. J Cardiovasc. Electrophysiol. 2001; 21:112-4
Morte improvvisa nei trials sullo scompenso cardiaco
Prevenire lo scompenso e le sue recidive

Risk of SCD in post-MI
Mortality risk in contemporary post-MI patients with EF ≤ 30% tends to increase as a function of time from last MI
Wilber D et al. Circulation 2004;109:1082-84
Prevenire lo scompenso e le sue recidive

Mortalità e disfunzione
VS nel post-infarto
0
10
20
30
40
50
mo
rta
lità
1 anno 5 anni
morte improvvisa mortalità totale
Tavazzi L Circulation 1997; 95: 1341-1345
Prevenire lo scompenso e le sue recidive

Morte improvvisa nella
miocardiopatia dilatativa
0123456789
10
n. even
t/1
00
pz/an
no
0-60 61-120mesi
mortalità totale morte scompenso o trap.
morte imp. morte imp. 3 mesi
3
mesi
Di Lenarda A Circulation 1998; 98: (suppl I): I-507
Prevenire lo scompenso e le sue recidive
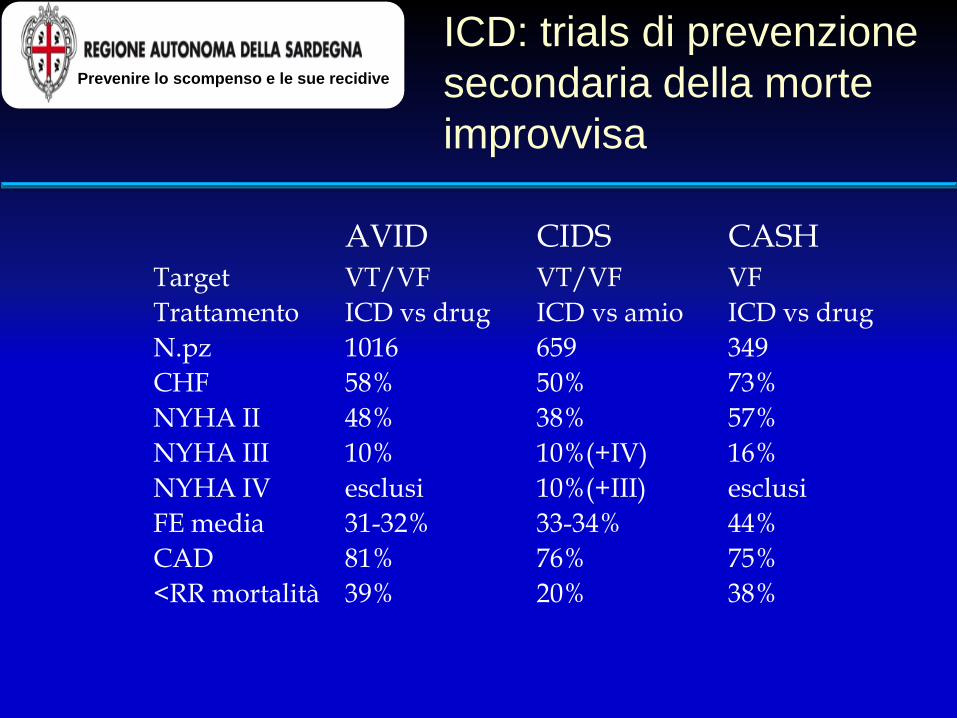
ICD: trials di prevenzione
secondaria della morte
improvvisa
AVID CIDS CASH Target VT/VF VT/VF VF
Trattamento ICD vs drug ICD vs amio ICD vs drug
N.pz 1016 659 349
CHF 58% 50% 73%
NYHA II 48% 38% 57%
NYHA III 10% 10%(+IV) 16%
NYHA IV esclusi 10%(+III) esclusi
FE media 31-32% 33-34% 44%
CAD 81% 76% 75%
<RR mortalità 39% 20% 38%
Prevenire lo scompenso e le sue recidive
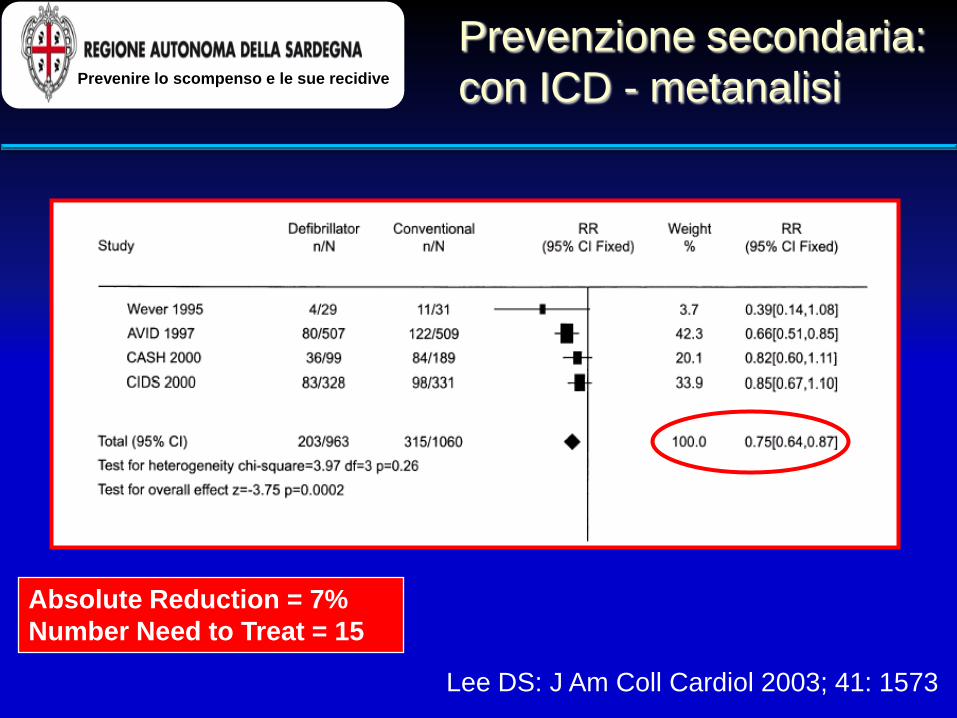
Effectiveness of ICDs in Preventing SD
A Meta Analysis – Secondary Prevention
Lee DS: J Am Coll Cardiol 2003; 41: 1573
Absolute Reduction = 7%
Number Need to Treat = 15
Prevenzione secondaria:
con ICD - metanalisi
Prevenire lo scompenso e le sue recidive
ACC Heart Failure Guidelines
Based on the 2009 Focused Update Incorporated Into the
ACCF/AHA 2005 guidelines for the Diagnosis and Management
of Heart Failure in Adults: A Report of the American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines
Developed in Collaboration With: International Society for Heart and Lung Transplantation
Jessup M. JACC 53, n. 15, 2009: 1343-1382
Patients With Reduced Left
Ventricular Ejection Fraction
A cardioverter-defibrillator (ICD) is recommended as secondary prevention to prolong survival in patients with current or prior symptoms of HF and reduced LVEF who have a history of cardiac arrest, ventricular fibrillation, or hemodynamically destabilizing ventricular tachycardia. NO CHANGE
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Secondary Prevention: Implantable Cardioverter-Defibrillator
Jessup M. JACC 53, n. 15, 2009: 1343-1382
ACC/AHA/HRS 2008 Guidelines
for Device-Based Therapy
of Cardiac Rhythm Abnormalities
Epstein A. JACC 51, 21, 2008: 2085-2105
Implantable Cardioverter-Defibrillators
secondary prevention
ICD indicated in survivors of cardiac arrest due to
ventricular fibrillation or hemodynamically unstable
sustained VT, after defining the cause of the event and
to excluding completely reversible causes.
ICD indicated in patients with structural heart disease
and spontaneous sustained VT, whether
hemodynamically stable or unstable.
ICD indicated in patients with syncope of undetermined
origin with clinically relevant, hemodynamically
significant sustained VT or VF induced at
electrophysiological study.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
ACC/AHA/HRS 2008 Epstein A. JACC 51, 21, 2008: 2085-2105
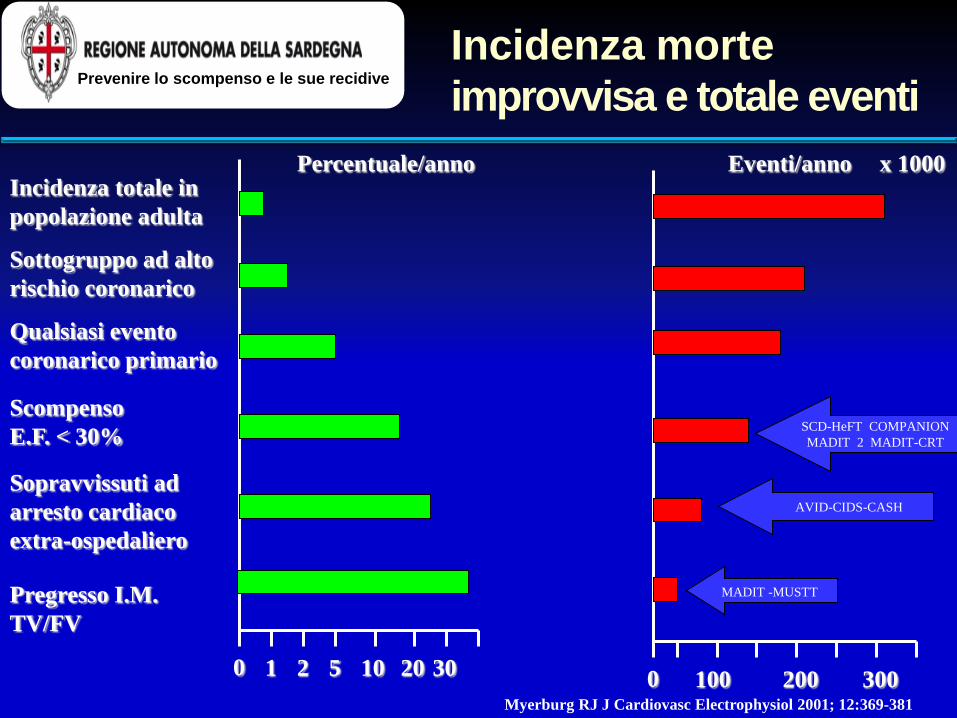
Incidenza morte
improvvisa e totale eventi
Percentuale/anno
0 1 2 5 10 20 30
Incidenza totale in
popolazione adulta
Sottogruppo ad alto
rischio coronarico
Qualsiasi evento
coronarico primario
Scompenso
E.F. < 30%
Sopravvissuti ad
arresto cardiaco
extra-ospedaliero
Pregresso I.M.
TV/FV
Eventi/anno
0 100 200 300
x 1000
Myerburg RJ J Cardiovasc Electrophysiol 2001; 12:369-381
MADIT -MUSTT
AVID-CIDS-CASH
SCD-HeFT COMPANION
MADIT 2 MADIT-CRT
Prevenire lo scompenso e le sue recidive

HF in Primary Prevention
Morbidity/Mortality Trials
NYHA
FE
I
II
III
IV
<30% <35%
NYHA
FE
I
II
III
IV
<30% <35%
IDIOPATHIC POST-MI
MADIT II (ICD) COMPANION (PM / ICD BiV) DEFINITE (ICD) SCD-HeFT (ICD)
©JM
Prevenire lo scompenso e le sue recidive
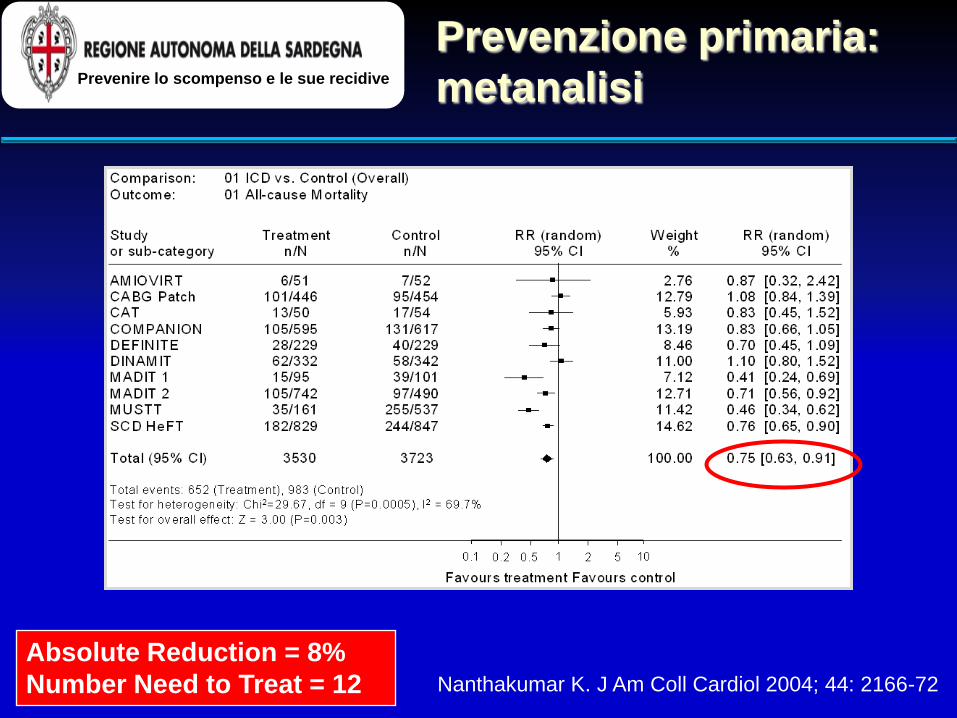
Nanthakumar K. J Am Coll Cardiol 2004; 44: 2166-72
Absolute Reduction = 8%
Number Need to Treat = 12
Prevenzione primaria:
metanalisi
Prevenire lo scompenso e le sue recidive
Patients With Reduced Left
Ventricular Ejection Fraction
ICD is recommended for primary prevention of sudden cardiac death to reduce total mortality in patients with nonischemic dilated cardiomyopathy or ischemic heart disease at least 40 days post-
myocardial infarction, LVEF ≤ 35%, NYHA II – III with optimal medical therapy, and who have reasonable expectation of survival with a good functional status for more than 1 year.
Modified
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Primary Prevention: Implantable Cardioverter-Defibrillator
Jessup M. JACC 53, 15, 2009: 1343-1382

ICD indicated in patients with LVEF < 35% due to prior MI who are at least 40 days post-MI and are in NYHA II or III.
ICD indicated in patients with LV dysfunction due to
prior MI who are at least 40 days post-MI, have LVEF < 30%, and are in NYHA I.
ICD indicated in patients with nonsustained VT due to
prior MI, LVEF < 40%, and inducible VF or sustained VT at electrophysiological study.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators
primary prevention post-MI
ACC/AHA/HRS 2008 Epstein A. JACC 51, 21, 2008: 2085-2105

ICD indicated in patients with nonischemic DCM who have an LVEF ≤ 35% and who are in NYHA II or III.
ICD is reasonable for patients with unexplained
syncope, significant LV dysfunction, and nonischemic DCM.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
Implantable Cardioverter-Defibrillators
primary prevention non ischemic DCM
ACC/AHA/HRS 2008 Epstein A. JACC 51, 21, 2008: 2085-2105
I IIa IIb III

ICD is reasonable for nonhospitalized patients awaiting transplantation.
ICD is reasonable for patients with cardiac sarcoidosis, giant cell myocarditis, or Chagas disease.
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
I IIa IIb III
I IIa IIb III
Implantable Cardioverter-Defibrillators
ACC/AHA/HRS 2008 Epstein A. JACC 51, 21, 2008: 2085-2105

ICD mortality reductions in primary prevention trials are equal
to or greater than those in secondary prevention trials.
37%
20%
54%60%
31%
41%
23%
36%
31%
0%
10%
20%
30%
40%
50%
60%
AVID
3
Years
CASH
2
years CIDS
3
years
MADIT
2
years MUSTT
5 years
Mo
rtali
ty R
ed
ucti
on
(%
)
MADIT II
3 years
Secondary
Prevention
Primary
Prevention
SCD-HeFT
5 years DEFINITE
3 years
COMPANION
1 years
Mortality reductions
with ICDs
Prevenire lo scompenso e le sue recidive

Sintomi di Scompenso Cardiaco + Ridotta Frazione d’Eiezione
Diuretico + ACE-I + ß-bloccante titolati alla stabilità clinica
Persistenza di segni e sintomi?
QRS>120 ms?
si
Considerare: CRT-P or CRT-D
Considerare: Digossina, idralazina/nitrati,
LVAD, trapianto
Aggiungere antagonista dell’aldosterone o ARB
Persistenza di segni e sintomi? no
si no
LVEF<35%?
si no
Considerare: ICD
Nessun ulteriore trattamento
si no
Strategy for use of drugs and devices in
symptomatic HF and systolic dysfunction
Dickstein K European Heart Journal 2008, 29: 2388-2442
Trials randomizzati hanno dimostrato nei paz.
con HF un significativo beneficio indotto
dall’ICD nella sopravvivenza libera da morte
improvvisa, sia in prevenzione primaria che
secondaria
Conclusioni
Prevenire lo scompenso e le sue recidive

La terapia di
resincronizzazione
cardiaca
Prevenire lo scompenso e le sue recidive

Elements of Cardiac Dyssynchrony
Atrio-
ventricular
Inter-
ventricular
Intra-
ventricular
Cazeau, et al. PACE 2003; 26[Pt. II]: 137–143
• riduce il tempo di riempimento diastolico
• prolunga il tempo di contrazione
• prolunga il rigurgito mitralico
• contrazione sistolica settale precoce
• dissinergia movimento parietale


• Intraventricular Activation • Organized ventricular
activation sequence • Coordinated septal and
free-wall contraction • Improved pumping
efficiency
Issues associated with heart failure
Mechanism II–ventricular resynchronization
Sinus node
AV node
Stimulation therapy
Conduction block



ACC Heart Failure Guidelines
Based on the 2009 Focused Update Incorporated Into the
ACCF/AHA 2005 guidelines for the Diagnosis and Management
of Heart Failure in Adults: A Report of the American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines
Developed in Collaboration With: International Society for Heart and Lung Transplantation
Jessup M. JACC 53, 15, 2009: 1343-1382
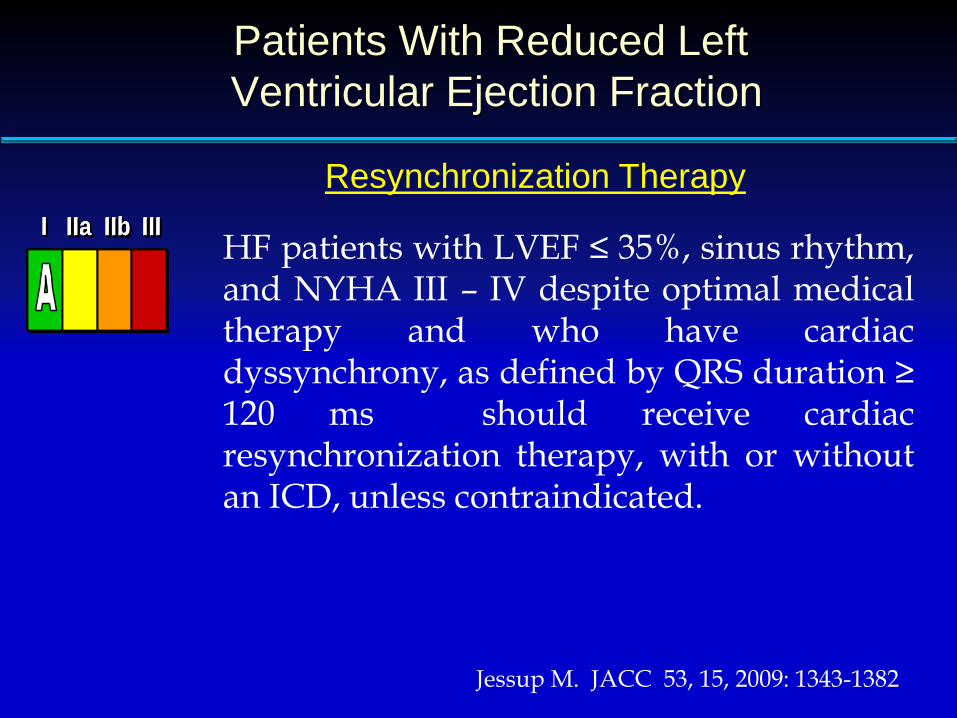
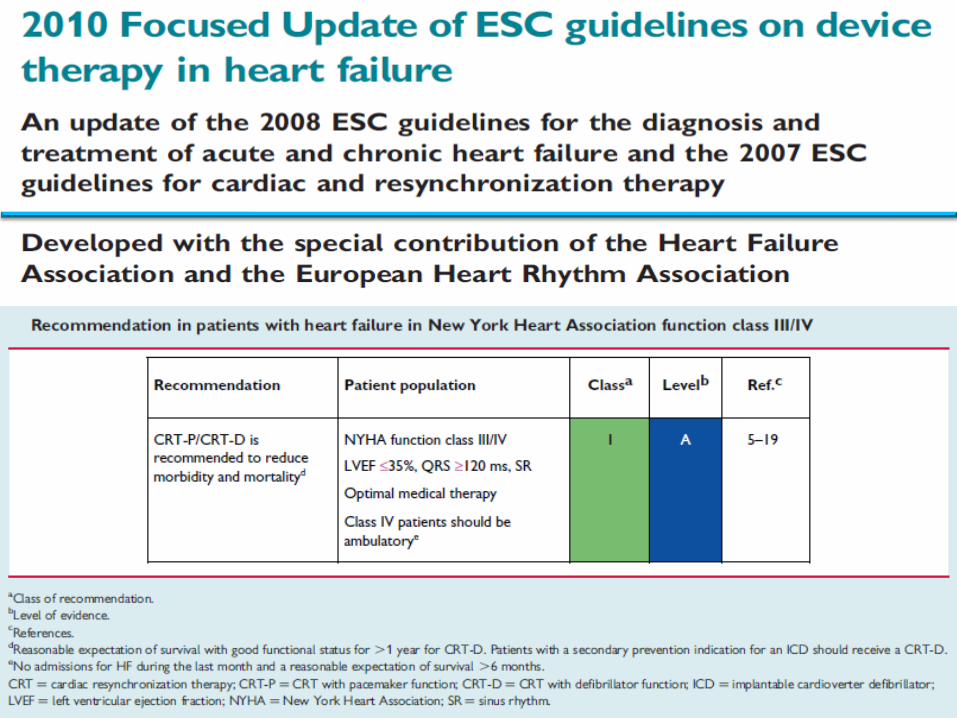
Patients With Reduced Left
Ventricular Ejection Fraction
HF patients with LVEF ≤ 35%, sinus rhythm, and NYHA III – IV despite optimal medical therapy and who have cardiac dyssynchrony, as defined by QRS duration ≥ 120 ms should receive cardiac resynchronization therapy, with or without an ICD, unless contraindicated.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Resynchronization Therapy
Jessup M. JACC 53, 15, 2009: 1343-1382

Sintomi di Scompenso Cardiaco + Ridotta Frazione d’Eiezione
Diuretico + ACE-I + ß-bloccante titolati alla stabilità clinica
Persistenza di segni e sintomi?
QRS>120 ms?
si
Considerare: CRT-P or CRT-D
Considerare: Digossina, idralazina/nitrati,
LVAD, trapianto
Aggiungere antagonista dell’aldosterone o ARB
Persistenza di segni e sintomi? no
si no
LVEF<35%?
si no
Considerare: ICD
Nessun ulteriore trattamento
si no
Treatment strategy for the use of drugs and devices in patients with symptomatic HF and systolic dysfunction
Dickstein K European Heart Journal 2008, 29: 2388-2442
ACC/AHA/HRS 2008 Guidelines
for Device-Based Therapy
of Cardiac Rhythm Abnormalities
May 2008

Cardiac Resynchronization Therapy* in
Patients With Severe Systolic Heart Failure
For patients with LVEF ≤ 35%, QRS duration ≥ 120 ms and sinus rhythm, CRT with or without ICD is indicated for the treatment of NYHA III - IV heart failure symptoms on optimal recommended medical therapy.
*All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
I IIaIIbIII
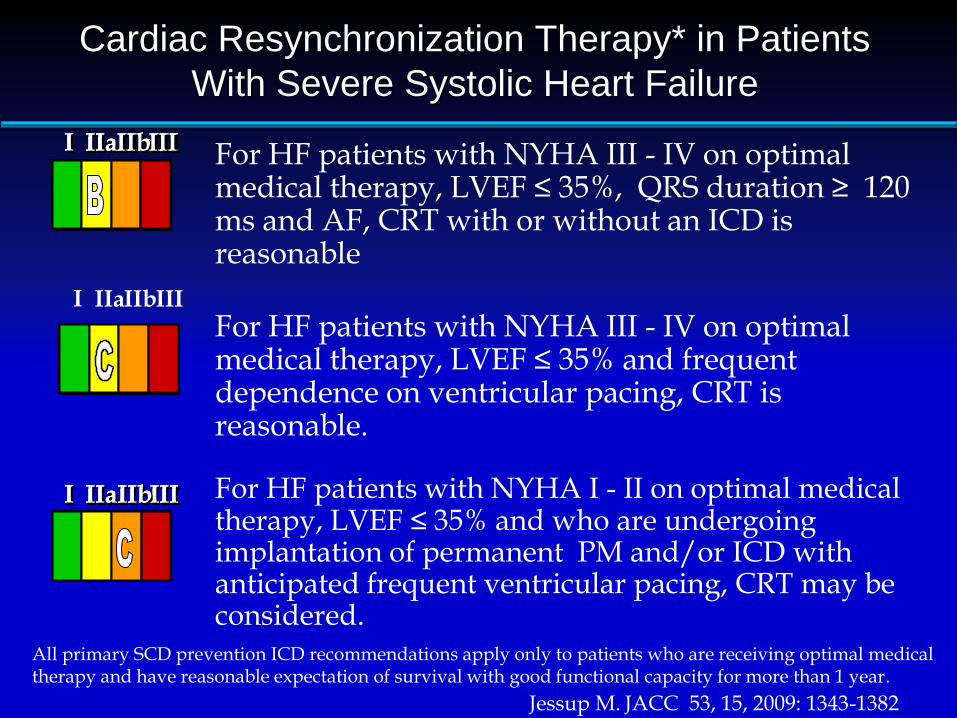
Cardiac Resynchronization Therapy* in Patients
With Severe Systolic Heart Failure
For HF patients with NYHA III - IV on optimal medical therapy, LVEF ≤ 35%, QRS duration ≥ 120 ms and AF, CRT with or without an ICD is reasonable
For HF patients with NYHA III - IV on optimal medical therapy, LVEF ≤ 35% and frequent dependence on ventricular pacing, CRT is reasonable.
For HF patients with NYHA I - II on optimal medical therapy, LVEF ≤ 35% and who are undergoing implantation of permanent PM and/or ICD with anticipated frequent ventricular pacing, CRT may be considered.
I IIa IIb III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
Jessup M. JACC 53, 15, 2009: 1343-1382

Cardiac Resynchronization Therapy* in
Patients With Severe Systolic Heart Failure
CRT is not indicated for asymptomatic patients with reduced LVEF in the absence of other indications for pacing.
CRT is not indicated for patients whose
functional status and life expectancy are limited predominantly by chronic noncardiac conditions.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
*All primary SCD prevention ICD recommendations apply only to patients who are receiving optimal medical therapy and have reasonable expectation of survival with good functional capacity for more than 1 year.


Trials randomizzati hanno dimostrato lo ICD riduce la
morte improvvisa nello HF, sia in prevenzione primaria
che secondaria
Trials randomizzati in paz. con HF in classe NYHA III–
IV hanno dimostrato una riduzione di eventi fatali e
non fatali con la CRT, con o senza ICD.
Trials randomizzati in paz. con HF in classe NYHA II
hanno dimostrato un beneficio della CRT, con o
senza ICD, sulla progressione di malattia e sulla
morbosità.
Conclusioni Prevenire lo scompenso e le sue recidive
Prevenire lo scompenso e le sue recidive
L’ultrafiltrazione utilizza apparecchiature assai simili a quelle
usate per l’emodialisi; Il sangue passa in un circuito veno-
venoso o artero-arterioso dove una membrana
semiperrmeabile filtrante lascia passare l’acqua e i soluti con
un peso molecolare inferiore ai 50000 Dalton;
•Deve essere presa in considerazione in pazienti selezionati con sovraccarico idrico (edema periferico e/o polmonare) e per correggere l’iponatriemia nei pazienti sintomatici refrattari alla terapia diuretica;
•Raccomandazione di Classe II a, livello di evidenza B
Ultrafiltrazione

Prevenire lo scompenso e le sue recidive
Rivascolarizzazione tramite PTCA (nelle forme ischemiche)
Utilizzo di dispositivi di assistenza ventricolare sinistra
(LVAD): le attuali indicazioni ne prevedono l’uso come
soluzione di ponte al trapianto in presenza di una miocardite
severa (Raccomandazione di Classe II a, Livello di evidenza C)
Terapia invasiva percutanea

Prevenire lo scompenso e le sue recidive
•
•Chirurgia coronarica
•Chirurgia valvolare
•Aneurismectomia ventricolare sinistra
•Trapianto cardiaco
Terapia chirurgica

















