
Endocrinologia e MetabolismoDipartimento di Medicina
SperimentaleSapienza Università di Roma
DIBATTITO N°4Gliflozine nel DM1
“Accusa”
Marco Giorgio Baroni
Il Prof Marco Giorgio Baroni dichiara di aver ricevuto negli ultimi due anni compensi o finanziamenti dalle seguenti Aziende Farmaceutiche e/o Diagnostiche:
- Sanofi- Novo Nordisk- Abbott- Takeda
Dichiara altresì il proprio impegno ad astenersi, nell’ambito dell’evento, dal nominare, in qualsivoglia modo o forma, aziende farmaceutiche e/o denominazione commerciale e di non fare pubblicità di qualsiasi tipo relativamente a specifici prodotti di interesse sanitario (farmaci, strumenti, dispositivi medico-chirurgici, ecc.).
Outline
• Abbiamo bisogno di terapie aggiuntive nel diabete di tipo 1?
• Ruolo SGLT2 inhibitors nel diabete di tipo 1
• Problemi aperti e richiesta alla corte
Abbiamo bisogno di terapie aggiuntive nel diabete di tipo 1?
• Problemi aperti della terapia insulinica nel Diabete tipo 1
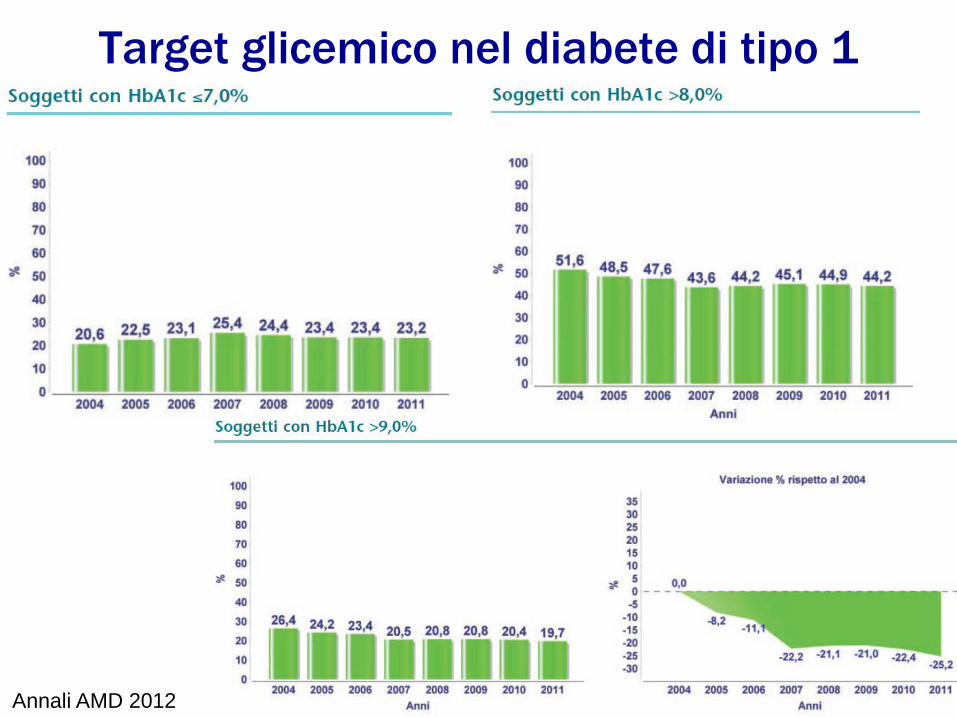
Target glicemico nel diabete di tipo 1
Annali AMD 2012
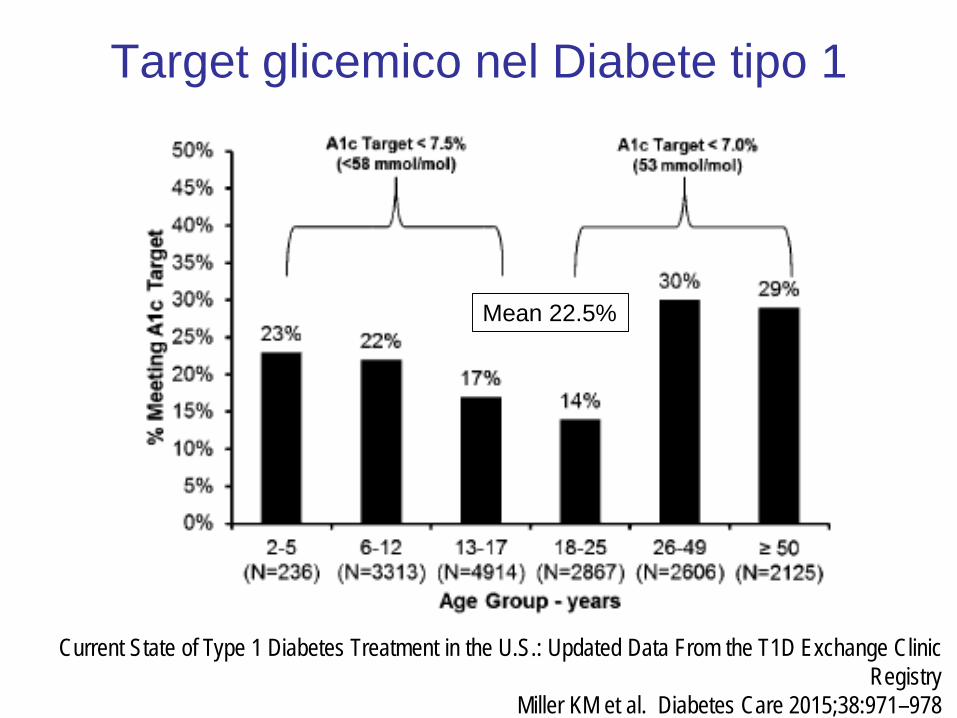
Target glicemico nel Diabete tipo 1
Current State of Type 1 Diabetes Treatment in the U.S.: Updated Data From the T1D Exchange Clinic Registry
Miller KM et al. Diabetes Care 2015;38:971–978
Mean 22.5%
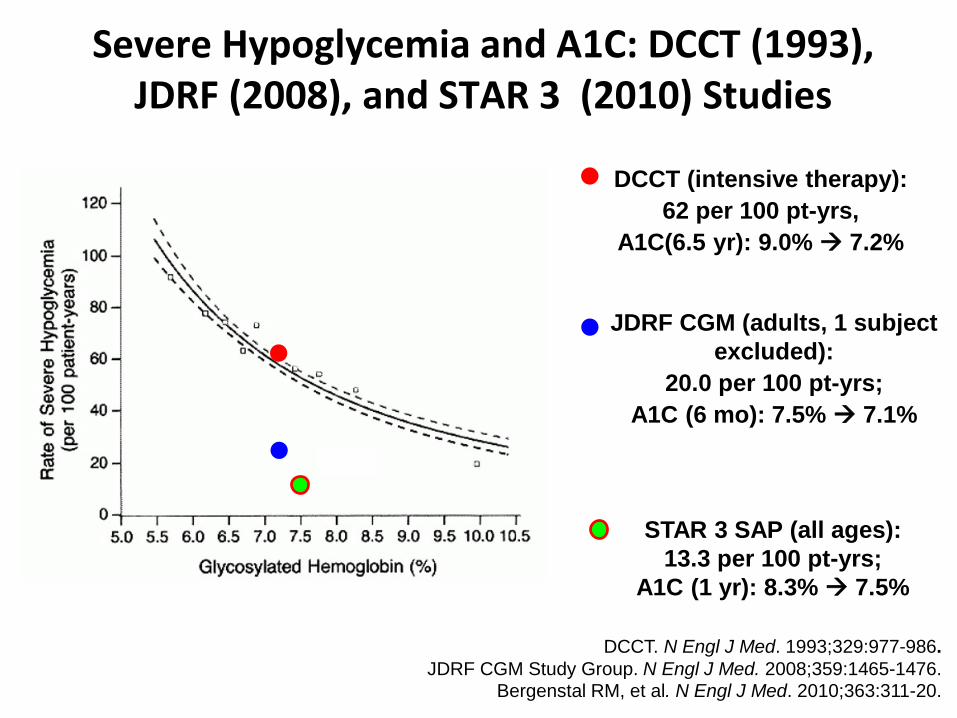
DCCT. N Engl J Med. 1993;329:977-986.JDRF CGM Study Group. N Engl J Med. 2008;359:1465-1476.
Bergenstal RM, et al. N Engl J Med. 2010;363:311-20.
JDRF CGM (adults, 1 subject excluded):
20.0 per 100 pt-yrs;A1C (6 mo): 7.5% 7.1%
DCCT (intensive therapy):62 per 100 pt-yrs,
A1C(6.5 yr): 9.0% 7.2%
STAR 3 SAP (all ages): 13.3 per 100 pt-yrs;
A1C (1 yr): 8.3% 7.5%
Severe Hypoglycemia and A1C: DCCT (1993), JDRF (2008), and STAR 3 (2010) Studies
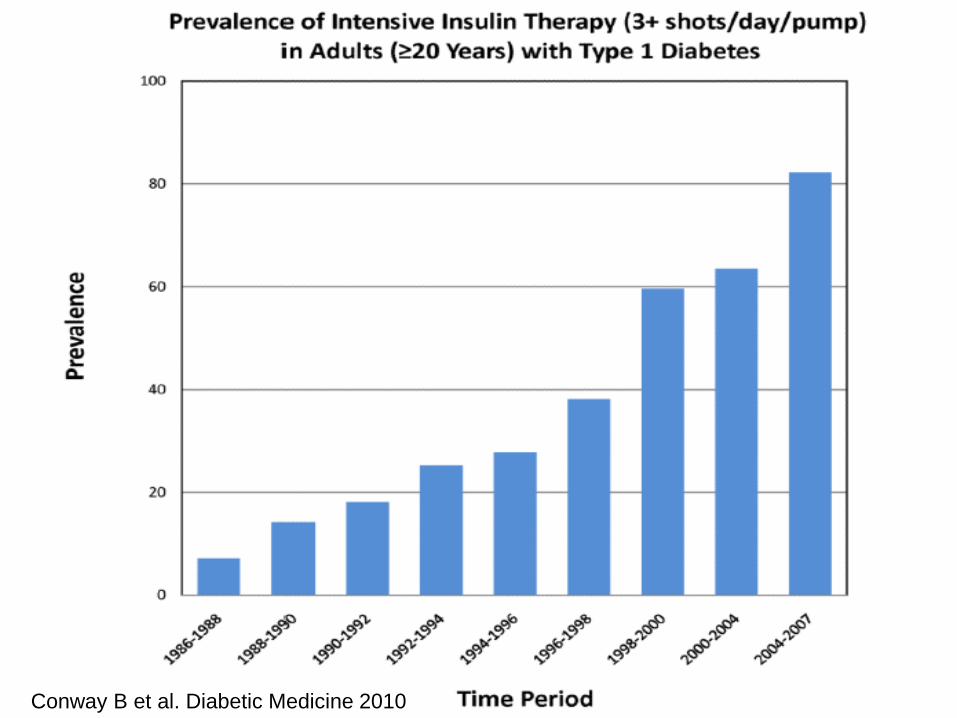
Conway B et al. Diabetic Medicine 2010
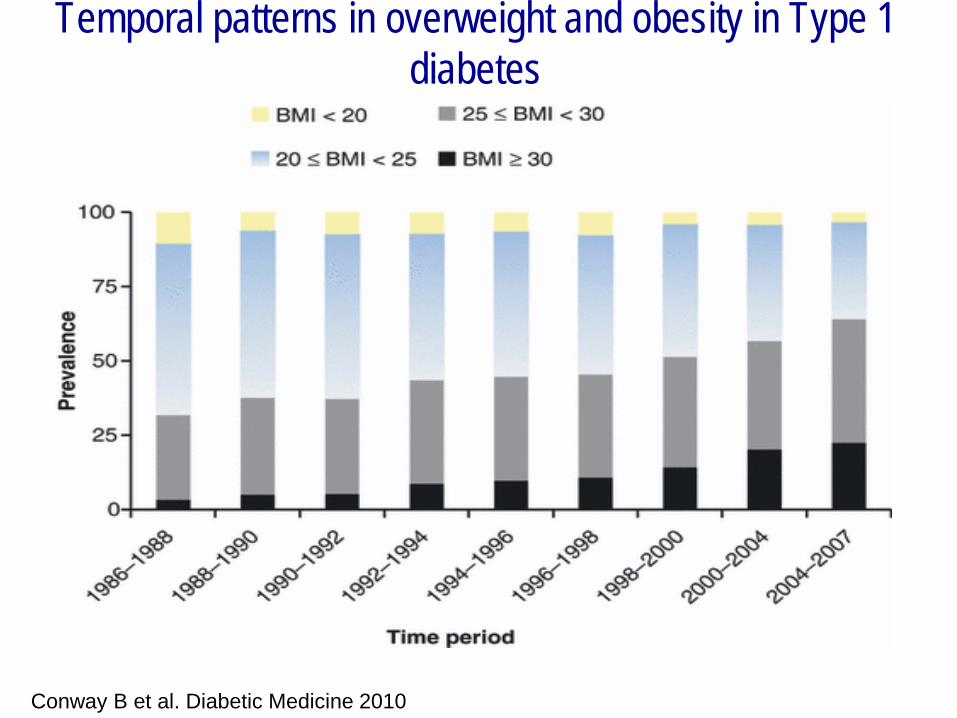
Temporal patterns in overweight and obesity in Type 1 diabetes
Conway B et al. Diabetic Medicine 2010
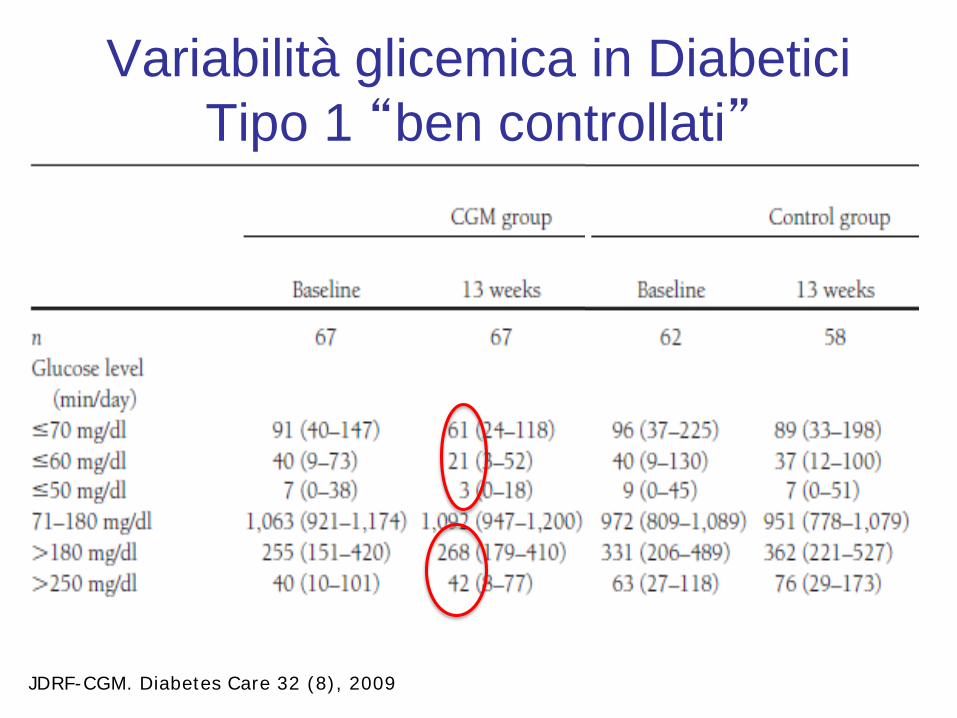
Variabilità glicemica in Diabetici Tipo 1 “ben controllati”
JDRF-CGM. Diabetes Care 32 (8), 2009
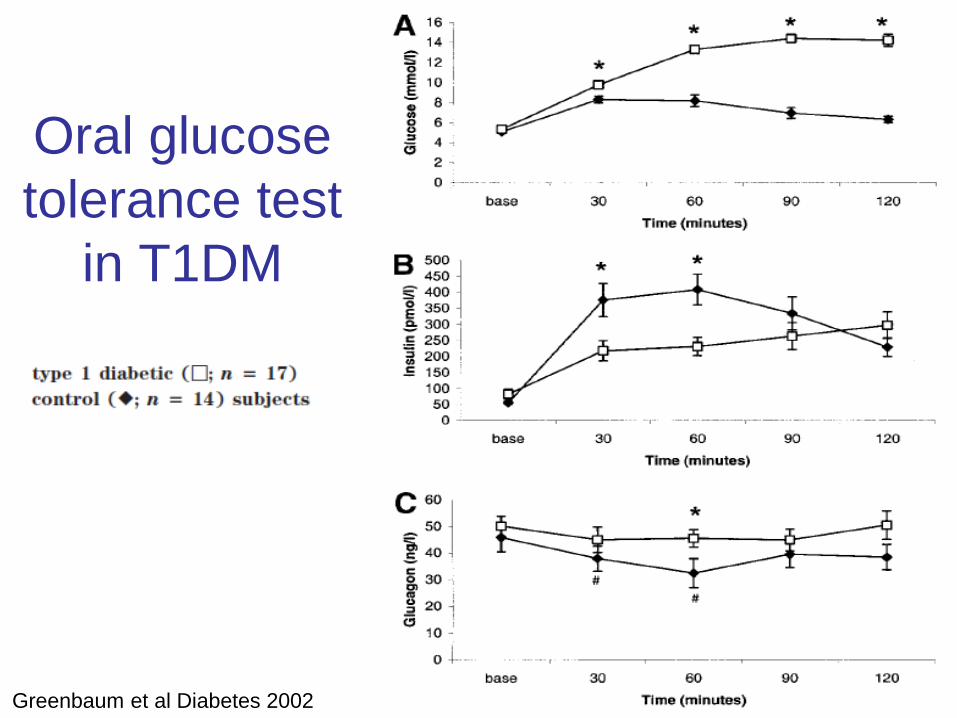
Oral glucosetolerance test
in T1DM
Greenbaum et al Diabetes 2002
Problemi aperti della terapia del diabete di tipo 1
• Target glicemico • Ipoglicemie• Aumento di peso• Variabilità glicemica• Iperglucagonemia• Compliance (dosi
ritardate/mancate/inerzia)
SGLT2i in type 1 diabetes
• Sodium-glucose co-transporter-2 (SGLT2) inhibitorsimpair renal glucose reabsorption, causing a substantialexcretion of glucose in urine.
• Since the mechanism of action of SGLT2 inhibitors isinsulin-independent, a significant effect of these drugs on glucose control should be expected if used in patientswith type 1 diabetes.
• The glucosuria and osmotic diuresis induced by thesedrugs are associated in type 2 diabetic patients with weight loss and blood pressure lowering of 2–4 mm Hg.
Potential effects og SGLT2i in type 1 diabetes
– Reduction in HbA1c without increasing insulin doses– Weight reduction– Blood pressure reduction– Protective effects on the kidney and cardiovascular
system?
– Hypoglycemia?– DKA?
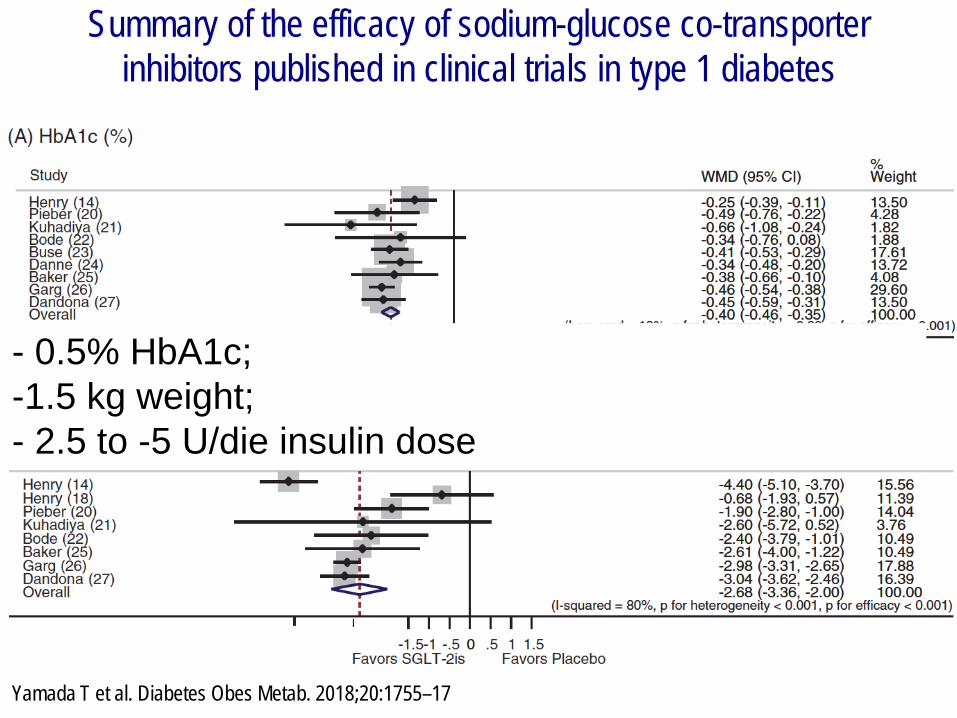
Summary of the efficacy of sodium-glucose co-transporterinhibitors published in clinical trials in type 1 diabetes
Yamada T et al. Diabetes Obes Metab. 2018;20:1755–17
- 0.5% HbA1c; -1.5 kg weight; - 2.5 to -5 U/die insulin dose
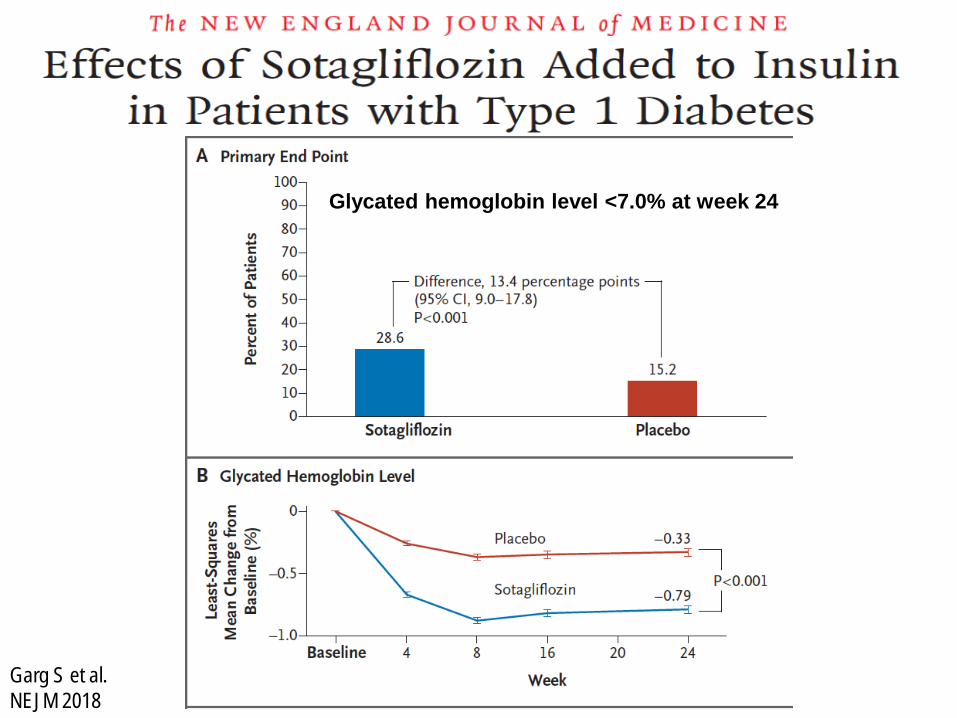
Garg S et al. NEJM 2018
Glycated hemoglobin level <7.0% at week 24
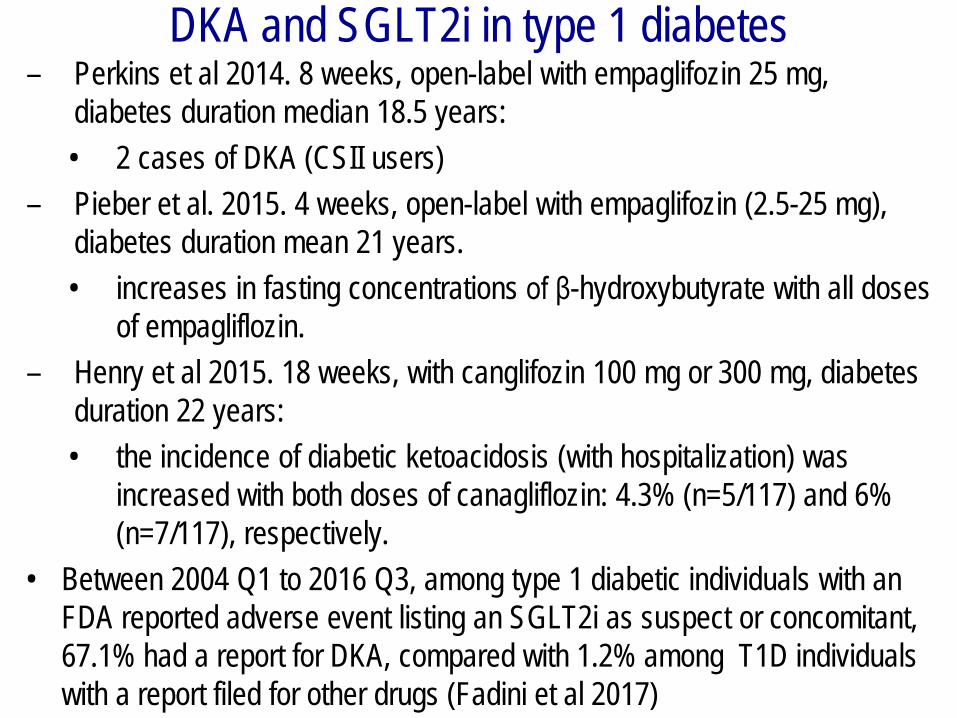
DKA and SGLT2i in type 1 diabetes– Perkins et al 2014. 8 weeks, open-label with empaglifozin 25 mg,
diabetes duration median 18.5 years: • 2 cases of DKA (CSII users)
– Pieber et al. 2015. 4 weeks, open-label with empaglifozin (2.5-25 mg), diabetes duration mean 21 years.• increases in fasting concentrations of β-hydroxybutyrate with all doses
of empagliflozin. – Henry et al 2015. 18 weeks, with canglifozin 100 mg or 300 mg, diabetes
duration 22 years: • the incidence of diabetic ketoacidosis (with hospitalization) was
increased with both doses of canagliflozin: 4.3% (n=5/117) and 6% (n=7/117), respectively.
• Between 2004 Q1 to 2016 Q3, among type 1 diabetic individuals with an FDA reported adverse event listing an SGLT2i as suspect or concomitant, 67.1% had a report for DKA, compared with 1.2% among T1D individualswith a report filed for other drugs (Fadini et al 2017)
eDKA
• DKA is traditionally defined by the triad of hyperglycemia (250 mg/dL), anion-gap acidosis, and increased plasma ketones
• Euglycemic DKA (eDKA), defined as DKA withoutmarked hyperglycemia (>200 mg/dl), is classicallyconsidered rare but this is perhaps a result of underrecognition and underreporting
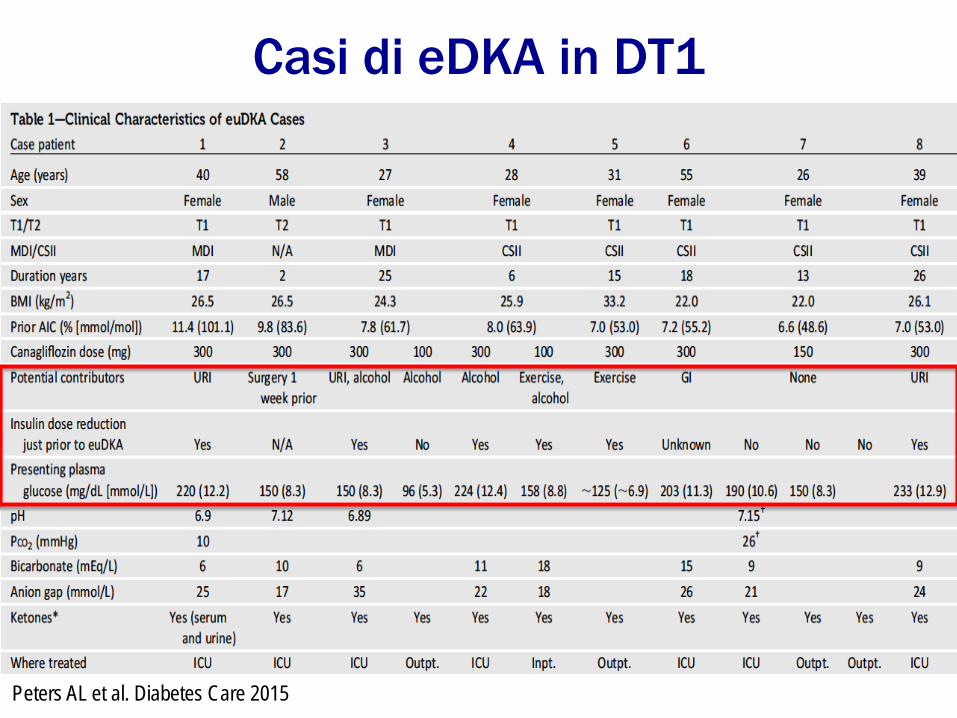
Casi di eDKA in DT1
Peters AL et al. Diabetes Care 2015
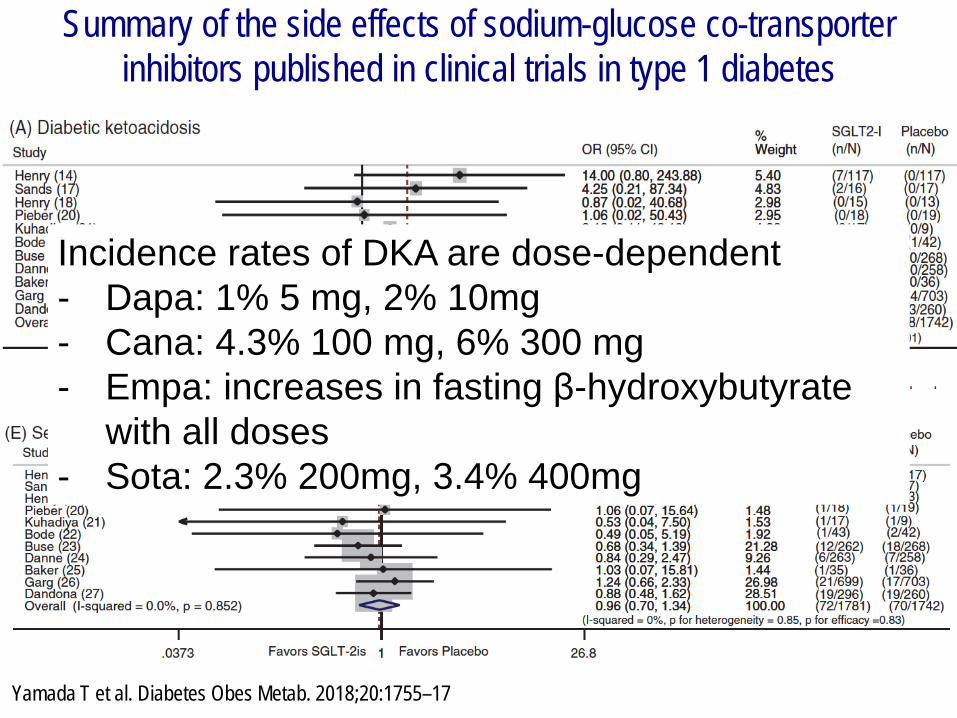
Summary of the side effects of sodium-glucose co-transporterinhibitors published in clinical trials in type 1 diabetes
Yamada T et al. Diabetes Obes Metab. 2018;20:1755–17
Incidence rates of DKA are dose-dependent- Dapa: 1% 5 mg, 2% 10mg- Cana: 4.3% 100 mg, 6% 300 mg- Empa: increases in fasting β-hydroxybutyrate
with all doses- Sota: 2.3% 200mg, 3.4% 400mg
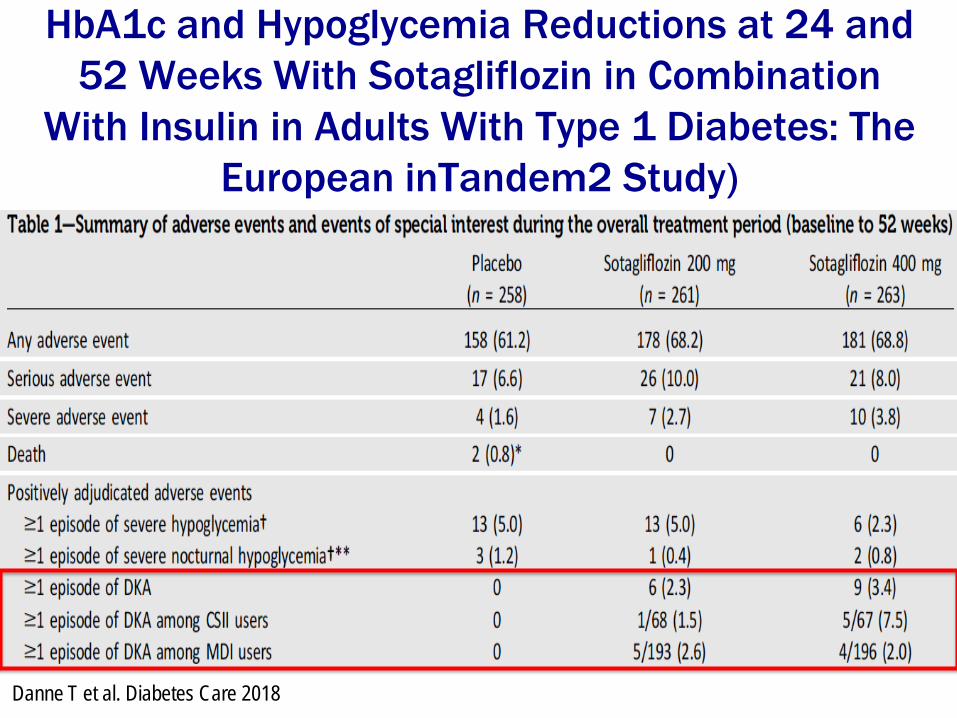
HbA1c and Hypoglycemia Reductions at 24 and 52 Weeks With Sotagliflozin in Combination
With Insulin in Adults With Type 1 Diabetes: The European inTandem2 Study)
Danne T et al. Diabetes Care 2018
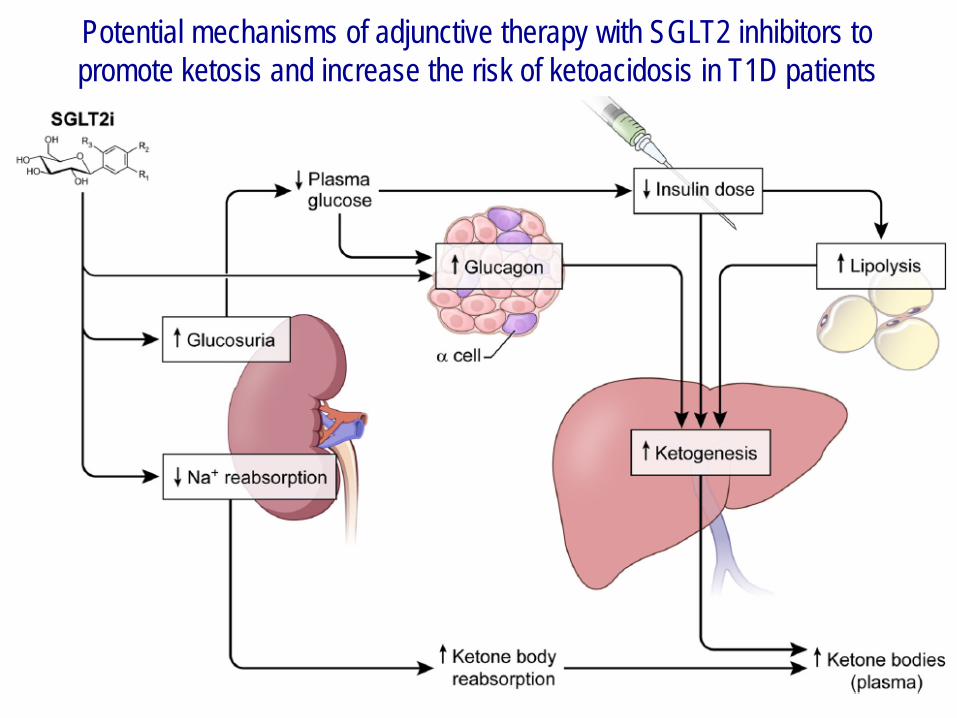
Potential mechanisms of adjunctive therapy with SGLT2 inhibitors to promote ketosis and increase the risk of ketoacidosis in T1D patients
Bonner C et al Nat Med 2015
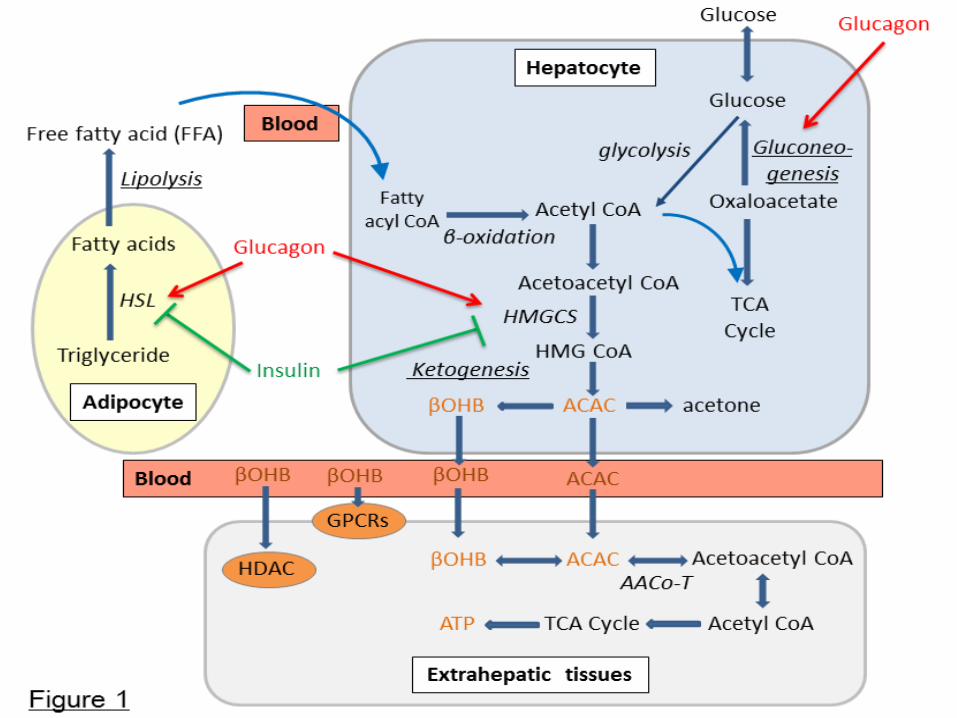
• In Acromegaly a shift from glucose to fatty acid oxidation after enhanced GH-induced lipolysis is a hallmark pathogenic feature
• SGLT2i increase plasma ketone levels through enhanced fat oxidation and increased synthesis as a result of an increased glucagon-to-insulin ratio
• Above the enhanced free fatty acid flux through GH induced lipolysis, the addition of empagliflozin further promoted hepatic ketogenesis due to increased glucagon-to-insulin ratio and decreased renal clearance of ketonebodies, resulting in euglycemic ketoacidosis
• Ketaoacidosis is determined by the additive effects of both conditions (i.e., uncontrolled GH excess and SGLT2 inhibition) on free fatty acid and ketone-body metabolism.
Possible causes of DKA with SGLT2i in T1DM
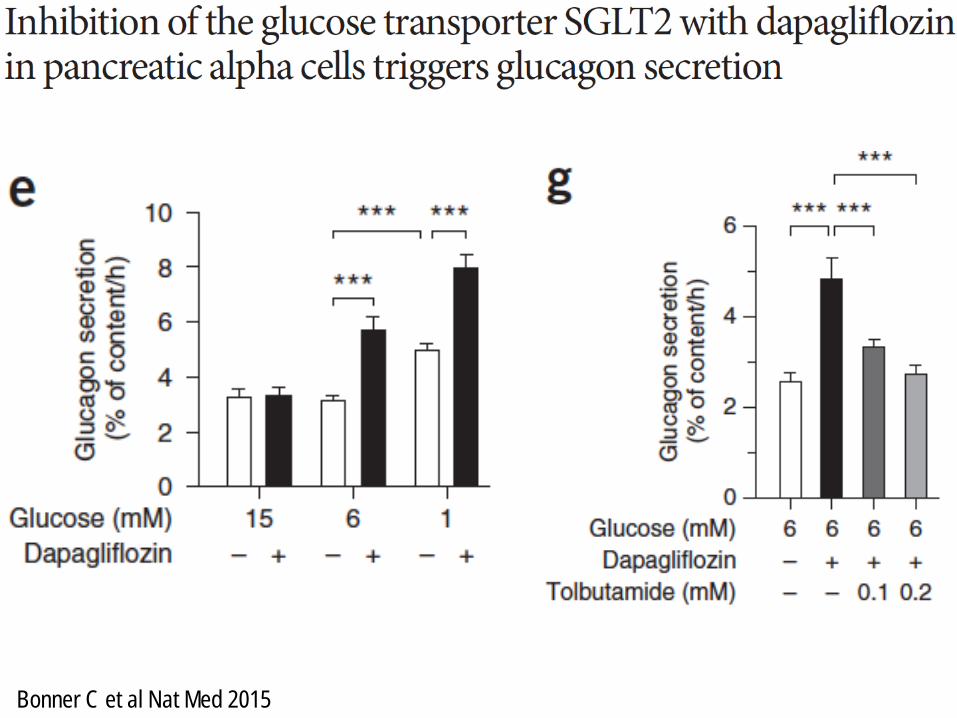
– Insulin dose reduction– SGLT2 is expressed in pancreatic alpha-cells, and SGLT2
inhibitors promote glucagon secretion– A decrease in the renal clearance of ketone bodies could
also increase the plasma ketone body levels• In the presence of risk factors (e.g., pump malfunctions,
carbohydrate restriction, increased alcohol consumption), reductions in the insulin-to-glucagon ratio in patients treatedwith SGLT2 inhibitors may increase susceptibility to DKA
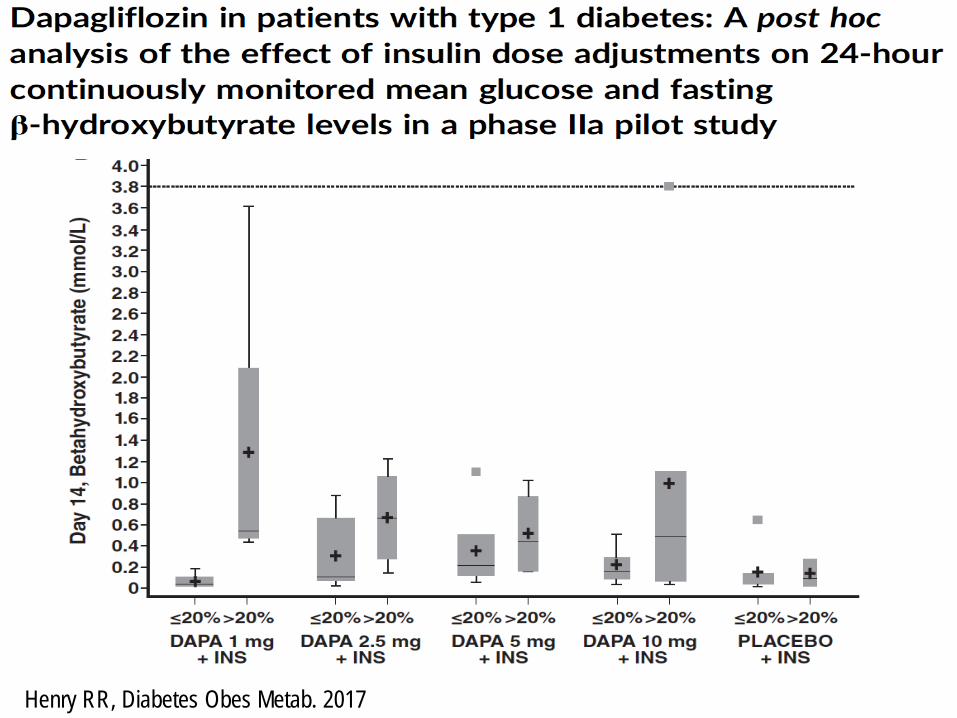
Henry RR, Diabetes Obes Metab. 2017
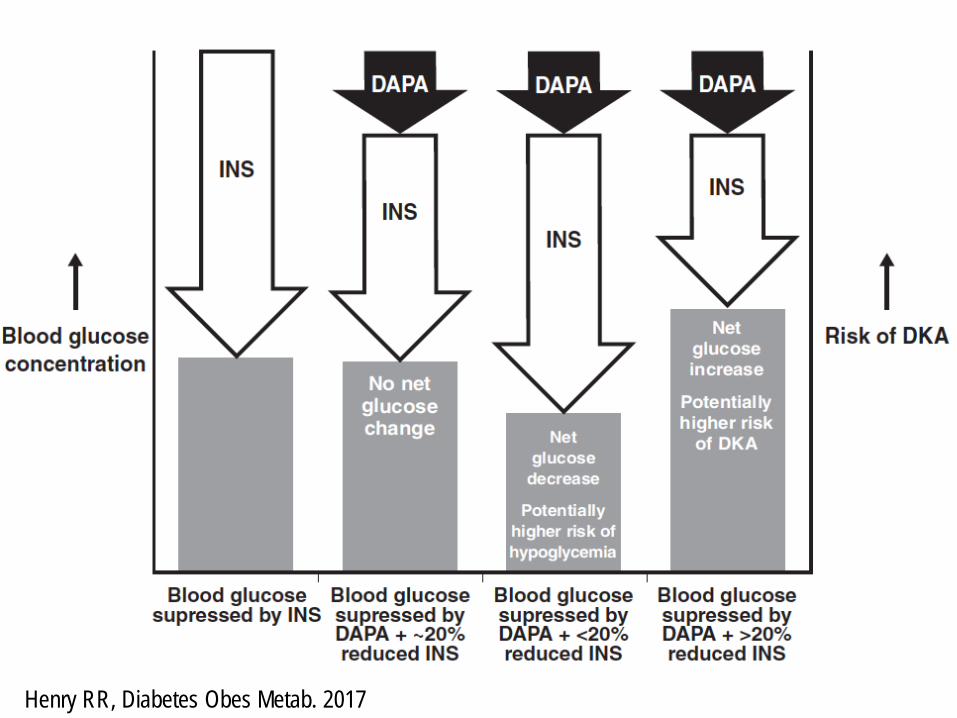
Henry RR, Diabetes Obes Metab. 2017
Conclusioni su SGLT2i nel T1DM• Il ruolo degli inibitori del SGLT2 come terapia add-on in
pazienti con diabete di tipo 1 è promettente, ma persistono questione aperte
• La relazione tra l’uso di SGLT2 inibitori e lo sviluppo di DKA nel DT1 deve essere valutata attentamente:– Serve un “punto di equilibrio” quando si decide di aggiustare la dose
insulinica in un paziente con DT1 che inizi SGLT2-i. – Il monitoraggio dei corpi chetonici deve essere considerato in pazienti
che hanno sintomi di DKA o sono in condizioni cliniche predisponenti (affaticamento, dolori addominali, digiuno, vomito, attività fisisca, uso di alcool, febbre, riduzione della terapia insulinica).
– Si deve assicurare un’adeguata dose insulinica con algoritmi clinici sul monitoraggio dei corpi chetonici, indipendentemente dalla glicemia
Richiesta di Sentenza
Si chiede la condanna degli inibitori del SGLT2:• ad anni 3 di ulteriori studi sugli effetti
collaterali• ad attività educazionale dedicata • allo sviluppo di algoritimi di terapia
insulinica dedicati







