

Alterazioni elettrolitiche
Rossana Berardi, Ancona
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Disordini elettrolitici in corso di terapia anti-EGFR
> Panitumumab vs. Cetuximab
> Nuovi anti-EGFR (Sym004)
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
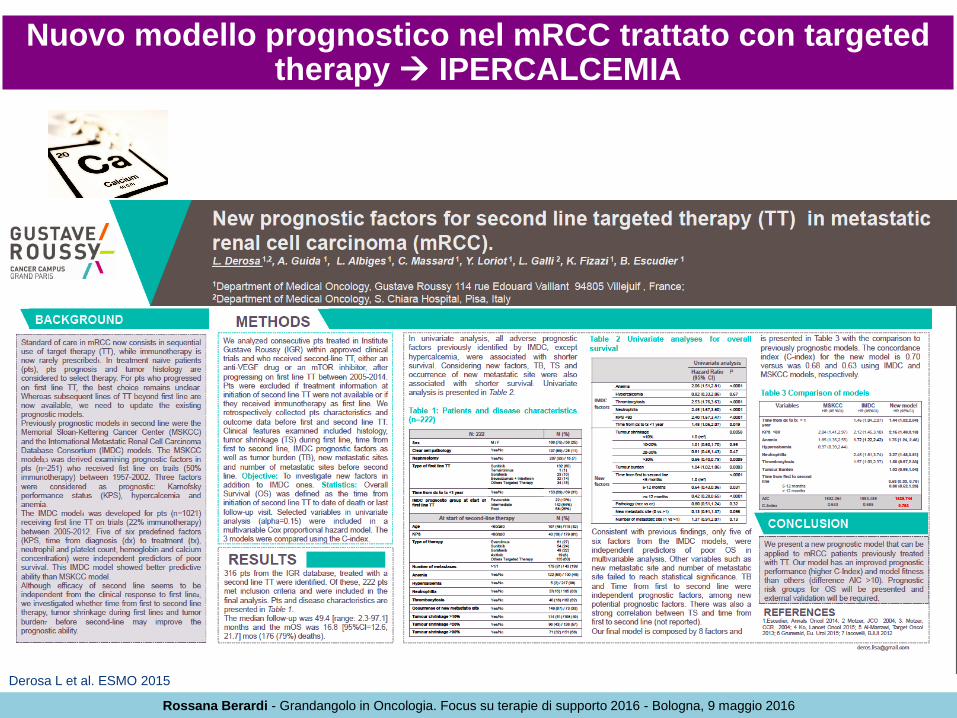
Nuovo modello prognostico nel mRCC trattato con targeted therapy IPERCALCEMIA
Derosa L et al. ESMO 2015
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
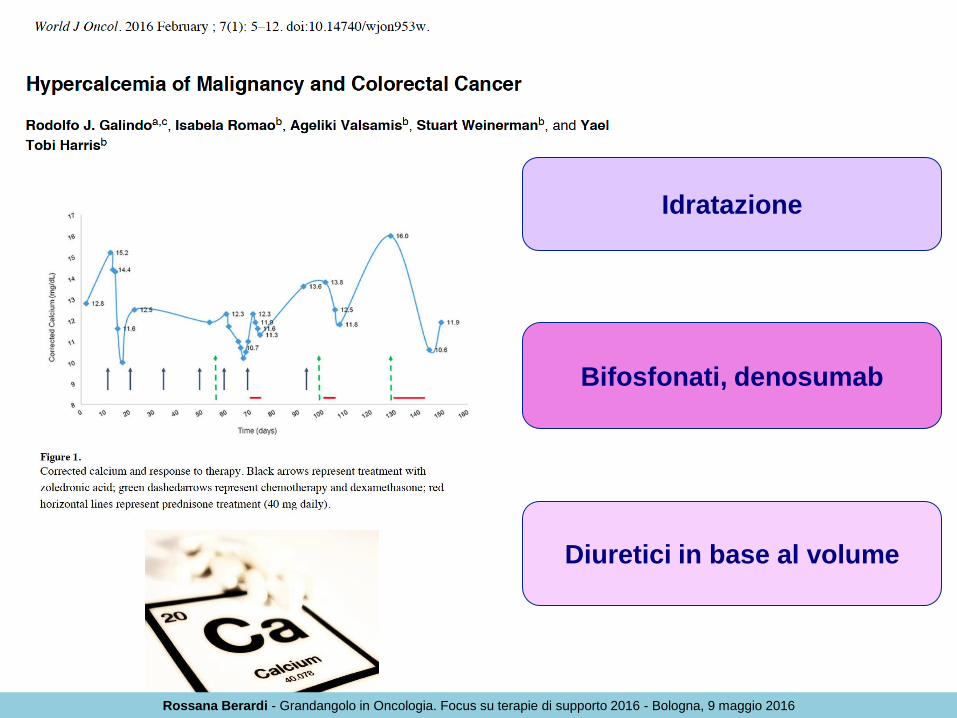
Idratazione
Diuretici in base al volume
Bifosfonati, denosumab
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
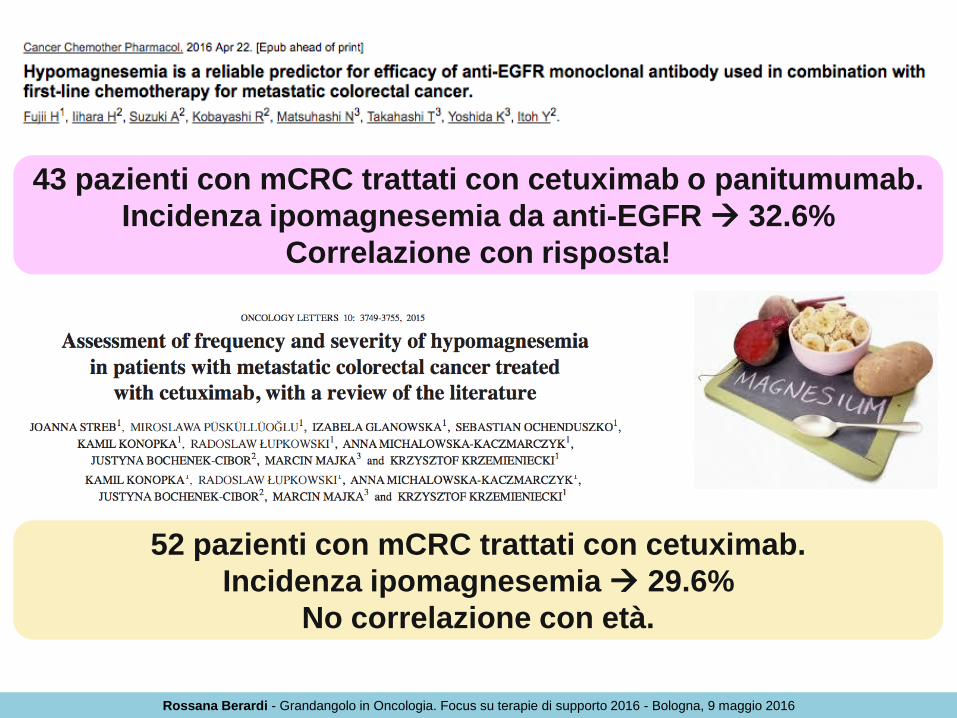
43 pazienti con mCRC trattati con cetuximab o panitumumab.
Incidenza ipomagnesemia da anti-EGFR 32.6%
Correlazione con risposta!
52 pazienti con mCRC trattati con cetuximab.
Incidenza ipomagnesemia 29.6%
No correlazione con età.
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Ipomagnesemia effetto di classe (anti-EGFR)
reversibile dopo settimane/mesi
Pertuzumab (>G1 = 14%) ≠ Trastuzumab
Studio ongoing prospettico per confermare
ipomagnesemia da pertuzumab in ca mammario HER-2+
Mancano studi prospettici per la terapia
dell’ipomagnesemia (supplementazione per os inefficace)
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Ipomagnesemia da panitumumab: frequente e correla con outcome!
Peeters M et al. ASCO GI 2016
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

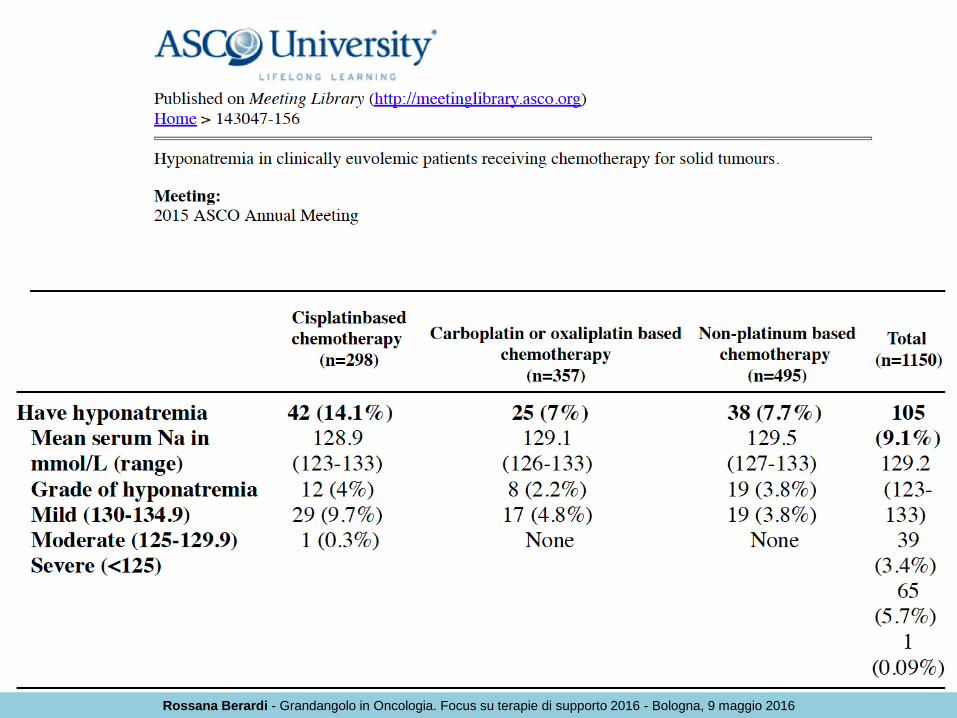
Iponatremia in oncologia: uno scenario in evoluzione
IERI…
Disorder Prevalence (%)
Intensive care patients 11–29.6
Elderly outpatients 7.2–11
Elderly inpatients 18–53
Heart failure 10.2–27
Cirrhosis 20.8–49.4
Cancer 3.7–47
Patients with pneumonia 8.1–27.9
Chronic kidney disease 13.6
Dialysis patients 29.3
Elderly patients with falls 9.1–13
Marathon runners 3–13
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Rates of hyponatremia in different cancers
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Surv
ival
pro
bab
ility
(%
) Time
Sodium ≥135 mEq/L
Sodium <135 mEq/L
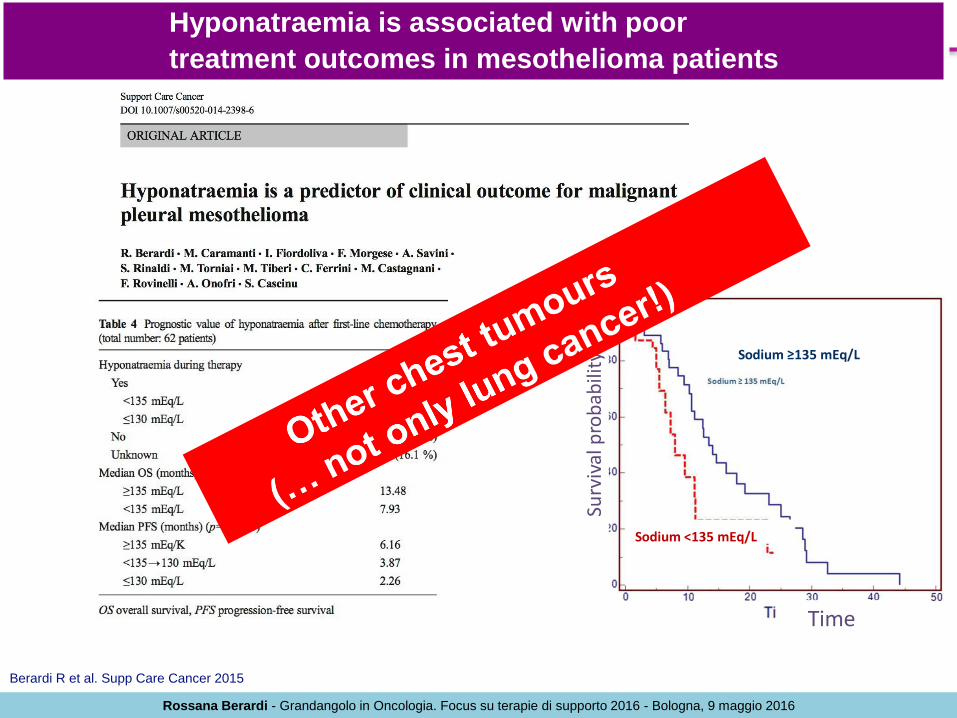
Hyponatraemia is associated with poor
treatment outcomes in mesothelioma patients
Berardi R et al. Supp Care Cancer 2015
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Surv
ival
pro
bab
ility
(%
) Time
Sodium ≥135 mEq/L
Sodium <135 mEq/L
Hyponatraemia is associated with poor
treatment outcomes in mesothelioma patients
Berardi R et al. Supp Care Cancer 2015
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
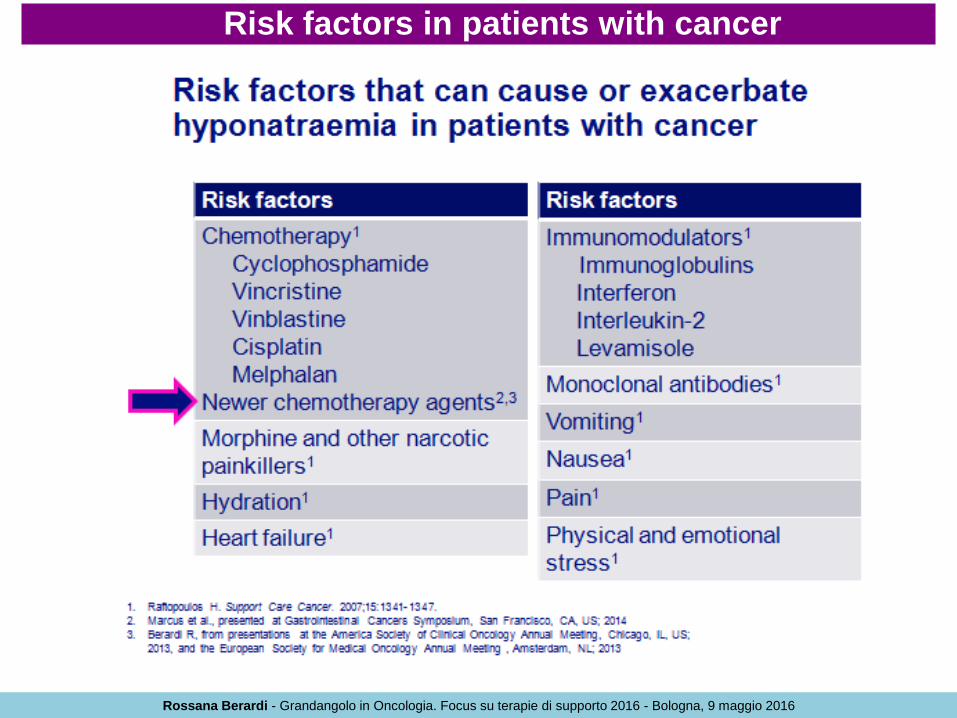
Risk factors in patients with cancer
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Essential criteria for the diagnosis of SIADH
• Hyponatraemia <135 mmol/L
• Plasma hypo-osmolality <275 mOsm/kg
• Urine osmolality >100 mOsm/kg
• Clinical euvolaemia
• No clinical signs of hypovolaemia (orthostatic decreases
in blood pressure, tachycardia, decreased skin turgor,
dry mucous membranes)
• No clinical signs of hypervolaemia (oedema, ascites)
• Increased urinary sodium excretion >40 mmol/L
with normal salt and water intake
• Absence of other potential causes of euvolaemic
hypo-osmolality
• Exclude recent diuretic use, renal disease, hypothyroidism
and hypocortisolism
1. Ellison DH, et al. N Engl J Med 2007;356:2064–2072.
2. Verbalis J, et al. Am J Med 2013;126(10 Suppl 1):S1–S42.
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
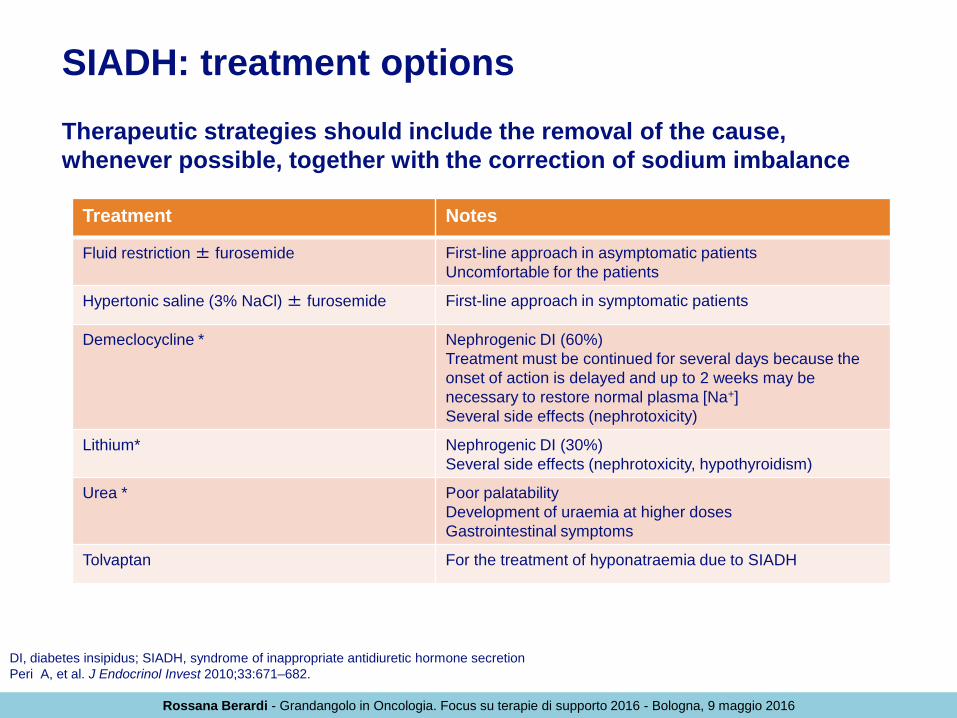
SIADH: treatment options
Therapeutic strategies should include the removal of the cause,
whenever possible, together with the correction of sodium imbalance
DI, diabetes insipidus; SIADH, syndrome of inappropriate antidiuretic hormone secretion
Peri A, et al. J Endocrinol Invest 2010;33:671–682.
Treatment Notes
Fluid restriction ± furosemide First-line approach in asymptomatic patients
Uncomfortable for the patients
Hypertonic saline (3% NaCl) ± furosemide First-line approach in symptomatic patients
Demeclocycline * Nephrogenic DI (60%)
Treatment must be continued for several days because the
onset of action is delayed and up to 2 weeks may be
necessary to restore normal plasma [Na+]
Several side effects (nephrotoxicity)
Lithium* Nephrogenic DI (30%)
Several side effects (nephrotoxicity, hypothyroidism)
Urea * Poor palatability
Development of uraemia at higher doses
Gastrointestinal symptoms
Tolvaptan For the treatment of hyponatraemia due to SIADH
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

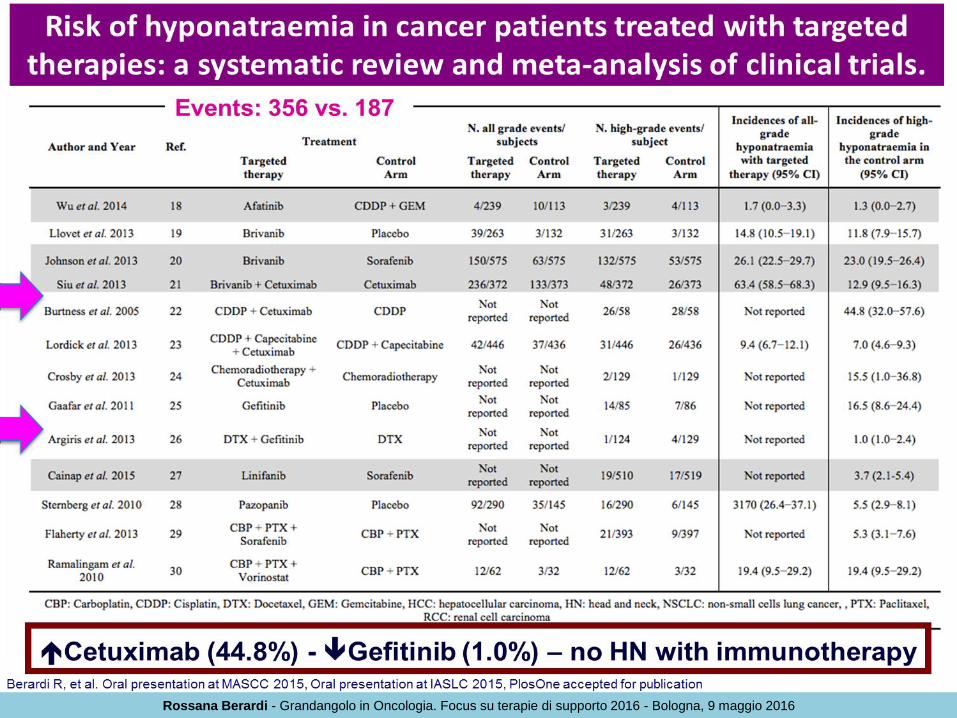
Aim of study: To investigate incidence and relative risk of hyponatraemia in
cancer patients treated with targeted therapies through an up-to-date
meta-analysis of available clinical trials
Berardi R, et al. Oral presentation at MASCC 2015, Oral presentation at IASLC 2015, PlosOne accepted for publication
The scientific literature regarding
hyponatraemia was extensively
reviewed using MEDLINE and
PubMed databases. Eligible
studies were selected according
to PRISMA statement.
Jadad score (mean):
3.7 (range 3–5)
Risk of hyponatraemia in cancer patients treated with targeted
therapies: systematic review and meta-analysis
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Risk of all-grade hyponatraemia with targeted agents
Berardi R, et al. Oral presentation at MASCC 2015, Oral presentation at IASLC 2015, PlosOne accepted for publication
Risk of high-grade hyponatraemia with targeted agents
Brivanib (RR=5.2), sorafenib (RR=2.4), vorinostat (RR=2.1)
anti-VEGF (RR=2.69) – anti-EGFR (RR=1.12)
Risk of hyponatraemia in cancer patients treated with targeted
therapies: systematic review and meta-analysis
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Survival time, months
Normalised to
136 + mEq/L
Not normalised
to 136 mEq/L
100
40
30
20
10
0 0 24
Normalised
Not Normalised
50 60
70
80
90 S
urv
iva
l, %
12
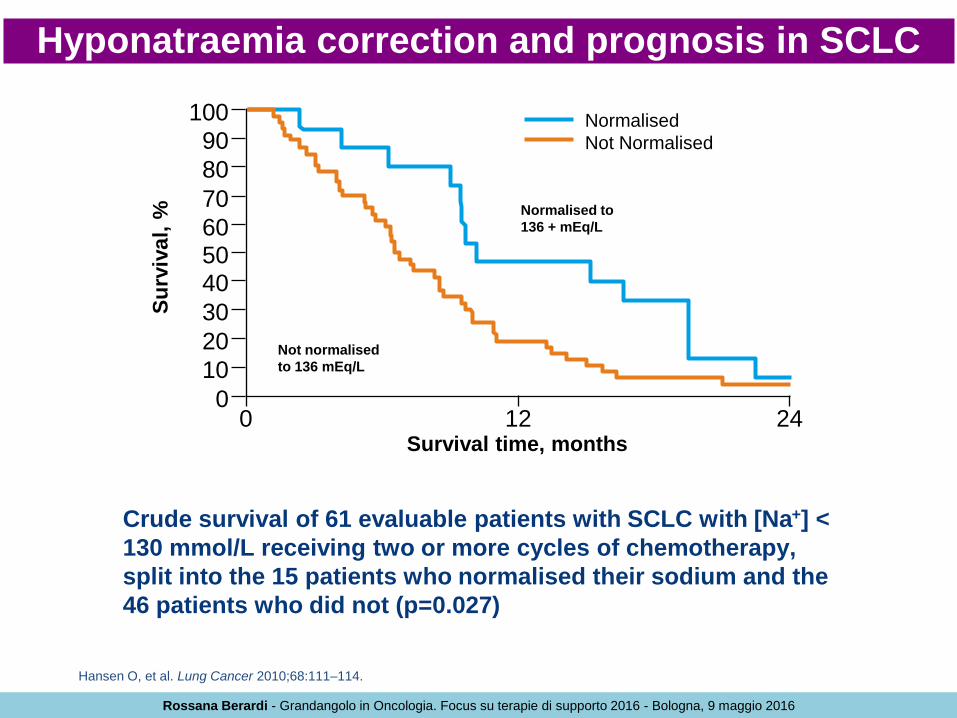
Hansen O, et al. Lung Cancer 2010;68:111–114.
Crude survival of 61 evaluable patients with SCLC with [Na+] <
130 mmol/L receiving two or more cycles of chemotherapy,
split into the 15 patients who normalised their sodium and the
46 patients who did not (p=0.027)
Hyponatraemia correction and prognosis in SCLC
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
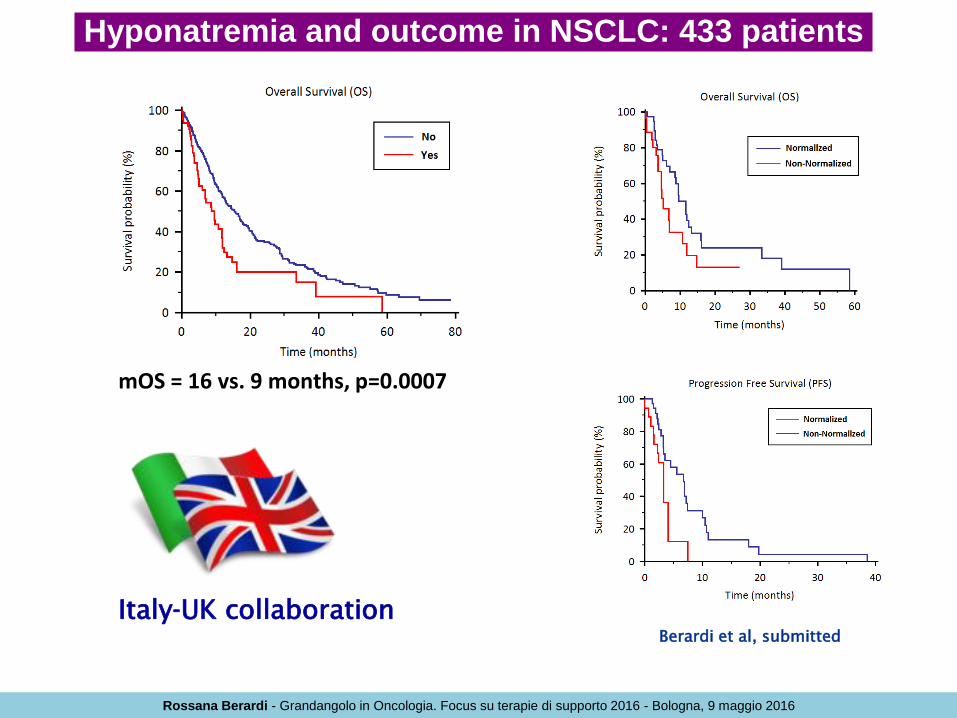
Berardi et al, submitted
Italy-UK collaboration
mOS = 16 vs. 9 months, p=0.0007
Hyponatremia and outcome in NSCLC: 433 patients
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Survival is the main, but not the only reason to treat SIADH…
Impact on patients’ QoL
and well-being
Increase of length of
hospitalization and readmission
rates
Delay of anticancer treatment
Costs increase
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

COSTS: 128% FOR
MODERATE HN 299% FOR SEVERE HN
Berardi et al, Supp Care Cancer 2015
Hyponatremia is a predictor of hospital length and cost of stay
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

Patient and disease characteristics at admission
SIADH, syndrome of inappropriate antidiuretic hormone secretion
De Las Peñas R, et al. Support Care Cancer 2016;24:499–507.
Patients N=35
Days to restore natraemia, n (%)
1–4 days
>4 days
Partial response
No response
18 (51)
13 (37)
3 (9)
1 (3)
Adverse events reported, n
Thirst
Polyuria
Dry mouth
Hepatic enzymes elevation
Others
Mild
9
6
4
2
0
Moderate
3
4
0
0
0
Severe
0
0
0
0
0
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

SIADH-related hyponatraemia in hospital day care units: clinical experience with tolvaptan
Treatment algorithm for hyponatraemia in cancer patients
SIADH, syndrome of inappropriate antidiuretic hormone secretion
De Las Peñas R, et al. Support Care Cancer 2016;24:499–507.
1. Administer tolvaptan until improvement in natraemia and then start chemotherapy. Can be administered jointly with chemotherapy under strict control of diuresis
2. Patient weight mL/h of SS 3%; with control of plasma [Na+] every 2 hours at start
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

SIADH-related hyponatraemia in hospital day care units: clinical experience with tolvaptan
Treatment algorithm for hyponatraemia in cancer patients
SIADH, syndrome of inappropriate antidiuretic hormone secretion
De Las Peñas R, et al. Support Care Cancer 2016;24:499–507.
1. Patients candidates for endocrine, biological, immune therapy, or exclusive symptomatic treatment
2. Patient weight mL/h of SS 3%; with control of plasma [Na+] every 2 hours at start
*Support treatments: fluid restriction; salt supplements
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016

ASSERT TRIAL: A prospective, observational study measuring
sodium improvement and outcomes in cancer patients treated for
moderate to severe hyponatremia secondary to SIADH
Lo studio si propone di raccogliere informazioni
scientifiche che aiutino a descrivere le caratteristiche dei
pazienti oncologici con SIADH, di definire le terapie per
correggere l’iponatremia nell’ambito della pratica clinica e di
validare/modificare le raccomandazioni attuali
Disegno dello studio
Osservazionale, prospettico, non interventistico, multicentrico
Centri partecipanti: 24 Centri Italiani
Dimensioni del campione: 80 pazienti (previsti 100 pazienti arruolati,
considerando dropout del 20%)
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016
Further improvements to be anticipated… - Prospective studies - Attention to standard cancer treatments
and newer targeted agents - Management strategies
Rossana Berardi - Grandangolo in Oncologia. Focus su terapie di supporto 2016 - Bologna, 9 maggio 2016







