

Carcinoma renale metastatico
Trattamento delle metastasi
Il punto di vista del chirurgo
Alberto Lapini

Nel 2015 erano attesi 10400 casi di tumore del parenchima renale.
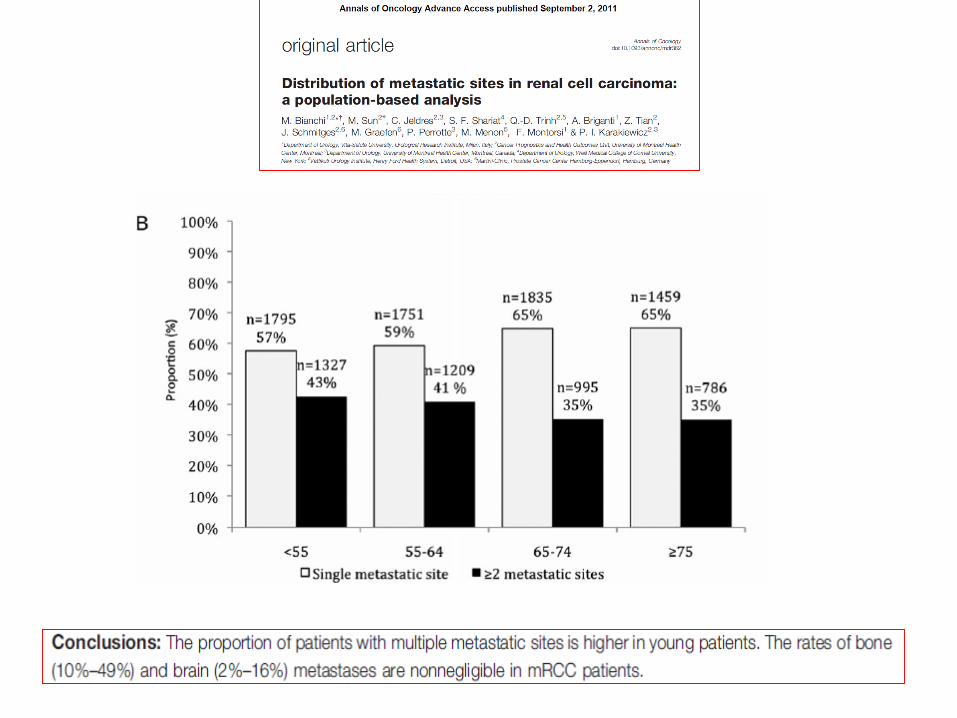
Nel 25-30% dei casi si tratta di una malattia metastatica alla diagnosi.Nel 5% dei casi è presente una metastasi
solitaria.
Le forme localizzate alla diagnosi danno metastasi in una percentuale che varia dal 35% al 65%


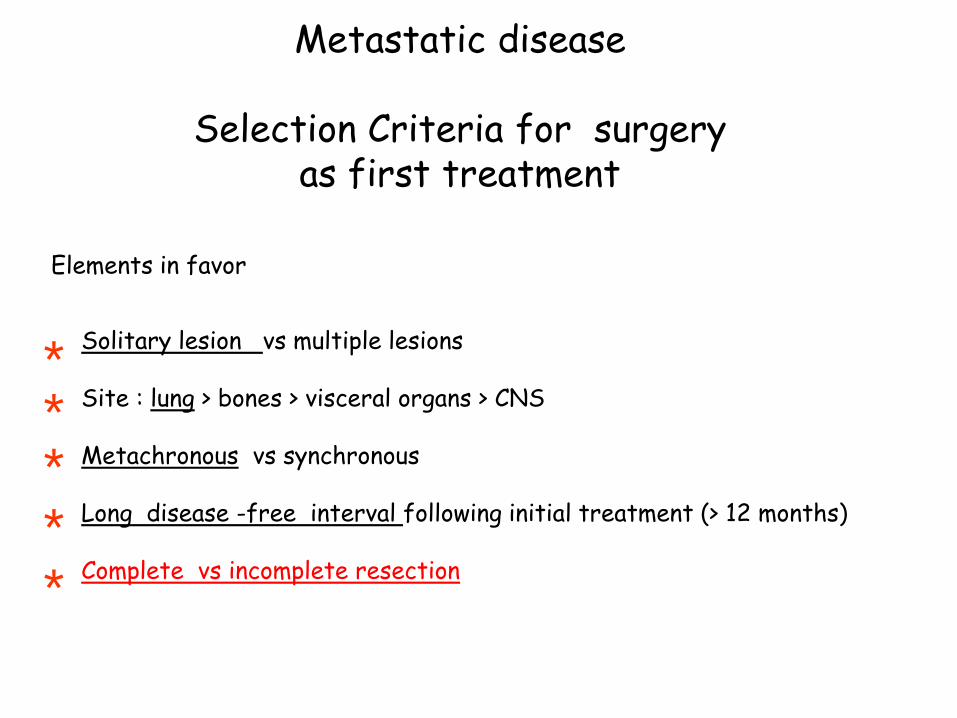
Metastatic disease
Selection Criteria for surgery as first treatment
Elements in favor
Solitary lesion vs multiple lesions
Site : lung > bones > visceral organs > CNS
Metachronous vs synchronous
Long disease -free interval following initial treatment (> 12 months)
Complete vs incomplete resection*
****

Lung only metastases
Non-lung only metastases
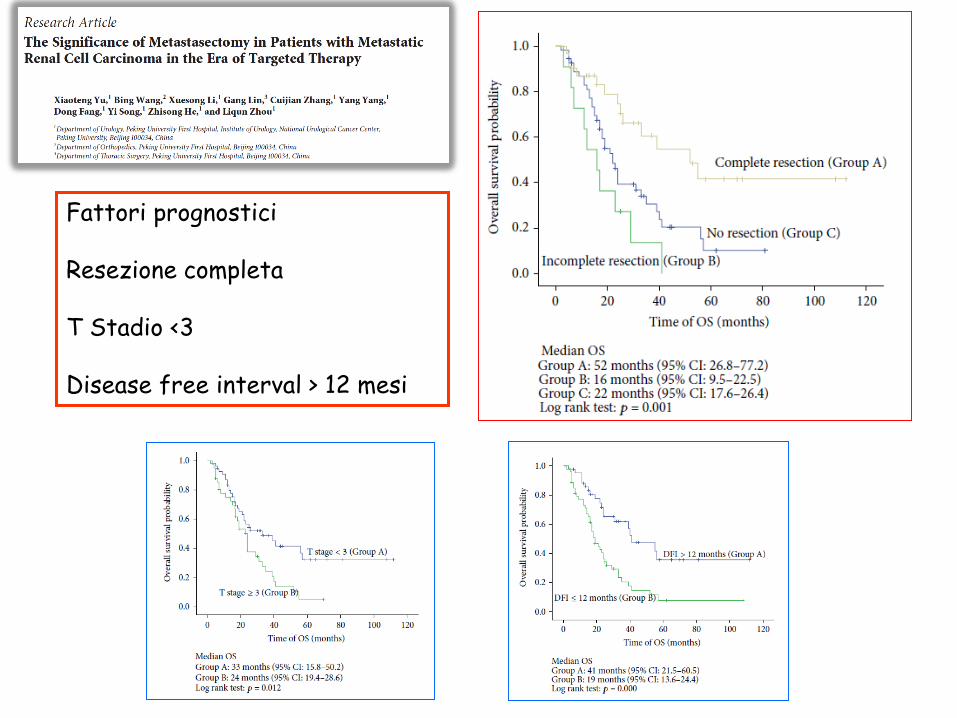
Fattori prognostici
Resezione completa
T Stadio <3
Disease free interval > 12 mesi
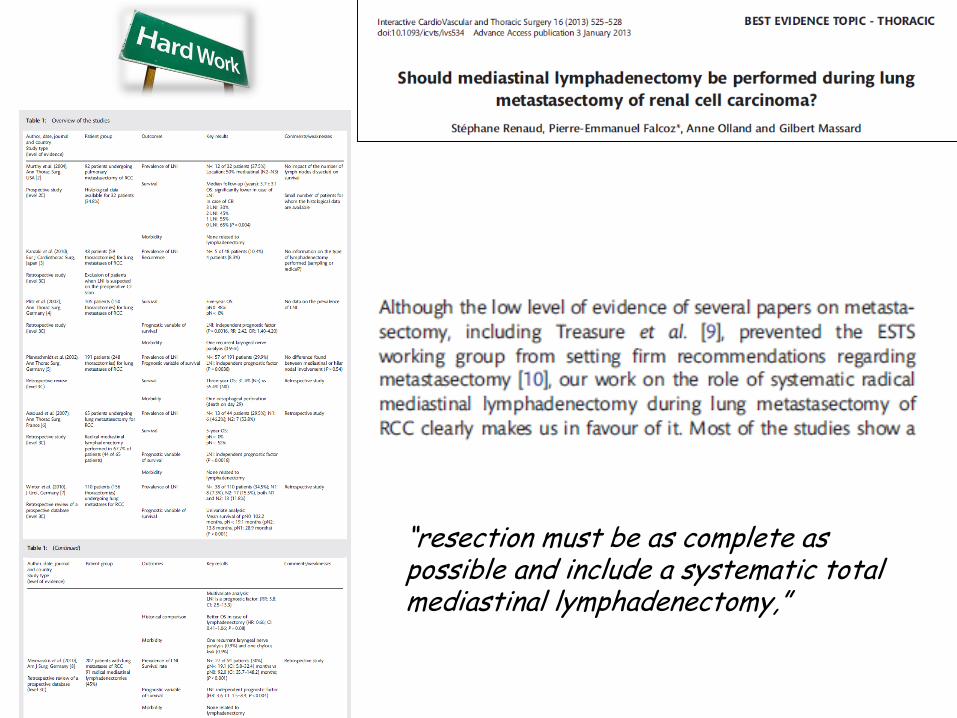
“resection must be as complete as possible and include a systematic total mediastinal lymphadenectomy,”
to operate or not to operate

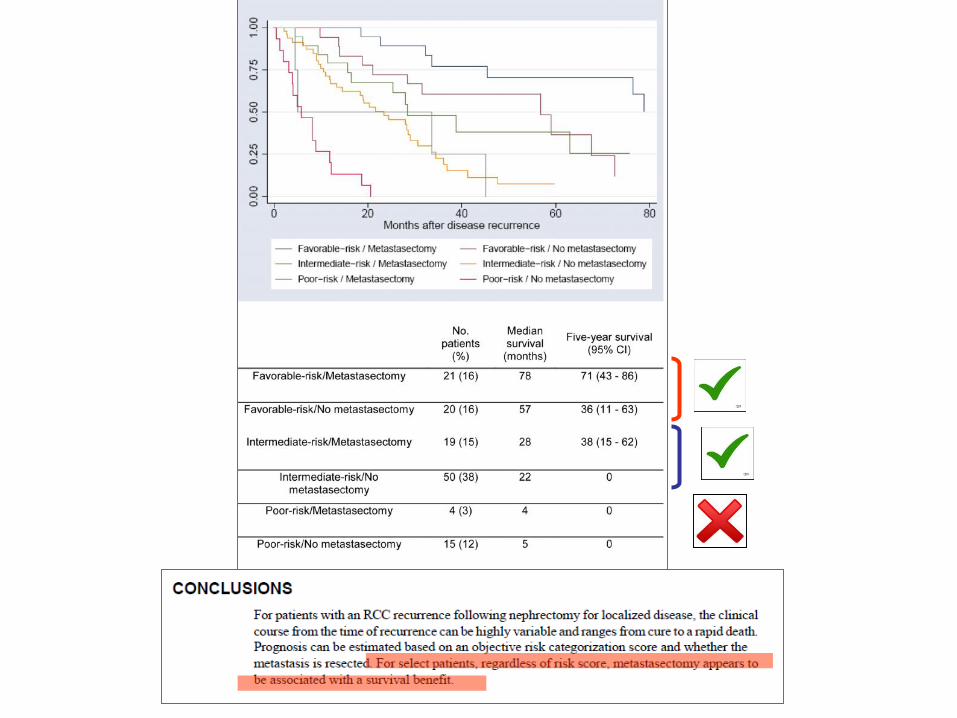
Parameters :
1-Serum Calcium > 10 mg/dL, 2-Hemoglobin less than age-specific lower
limit of normal3-Serum LDH > 300 U/L.
4-Karnofsky < 80%5-Time from nephrectomy to recurrence <
12 months
One point was assigned for each adverse parameter met, up to a maximum of 5 points.
Risk category : favorable-risk (0 points) intermediate-risk (1–2points)poor-risk (3–5 points)
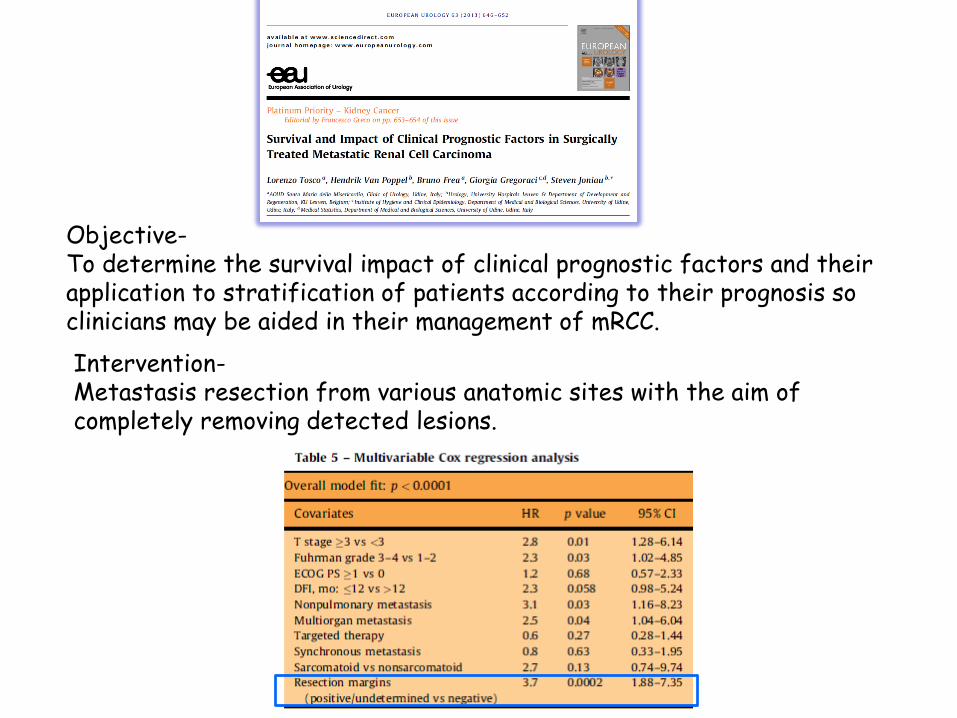
Objective-To determine the survival impact of clinical prognostic factors and theirapplication to stratification of patients according to their prognosis so clinicians may be aided in their management of mRCC.
Intervention-Metastasis resection from various anatomic sites with the aim of completely removing detected lesions.
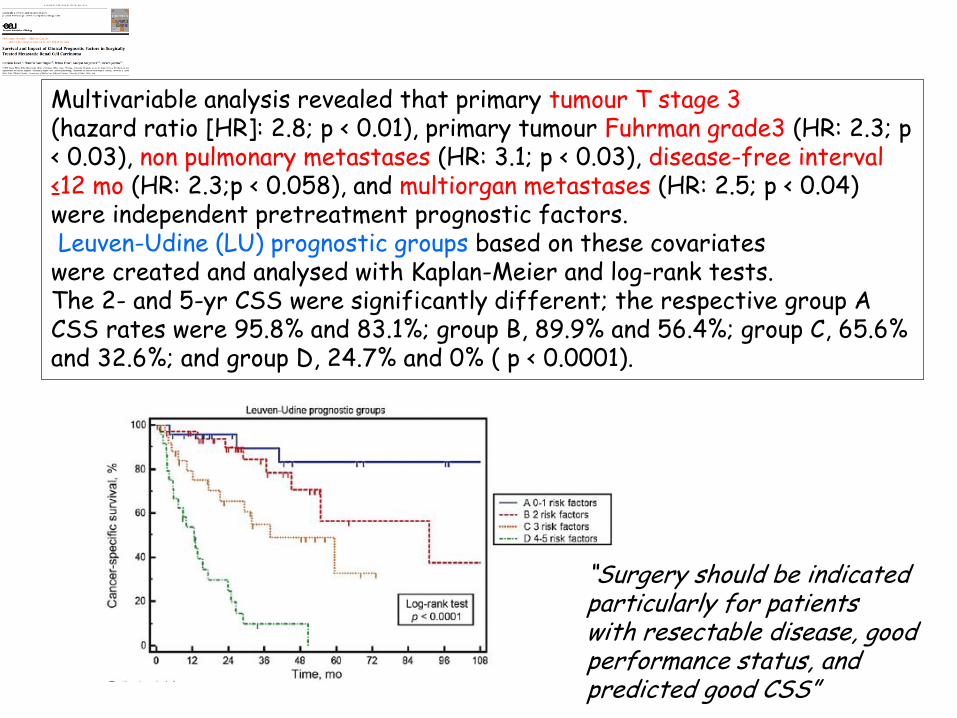
Multivariable analysis revealed that primary tumour T stage 3(hazard ratio [HR]: 2.8; p < 0.01), primary tumour Fuhrman grade3 (HR: 2.3; p < 0.03), non pulmonary metastases (HR: 3.1; p < 0.03), disease-free interval ≤12 mo (HR: 2.3;p < 0.058), and multiorgan metastases (HR: 2.5; p < 0.04) were independent pretreatment prognostic factors.Leuven-Udine (LU) prognostic groups based on these covariates
were created and analysed with Kaplan-Meier and log-rank tests. The 2- and 5-yr CSS were significantly different; the respective group A CSS rates were 95.8% and 83.1%; group B, 89.9% and 56.4%; group C, 65.6% and 32.6%; and group D, 24.7% and 0% ( p < 0.0001).
“Surgery should be indicated particularly for patientswith resectable disease, good performance status, andpredicted good CSS”

December 1996
May 2008 October 2011

Dicembre 2011: intervento di enucleazione renale robotica
E.I.: ca renale a cellule chiare, G3, pT1 ( 2,4 x 2 x1 cm)
!!La paziente è attualmente libera da malattia!!
Febbraio 2016
Anche se nel 2013 ha eseguito tiroidectomia per metastasi
da RCC e contemporaneamente sono apparse 2 nodularità
della testa del pancreas di circa 1 cm di diametro .
Rifiutando un nuovo intervento opta per trattamento con Tki
che determina la scomparsa dei noduli .
Interrompe terapia ad aprile 2014 per tossicità ematologica

Riprende terapia !!!
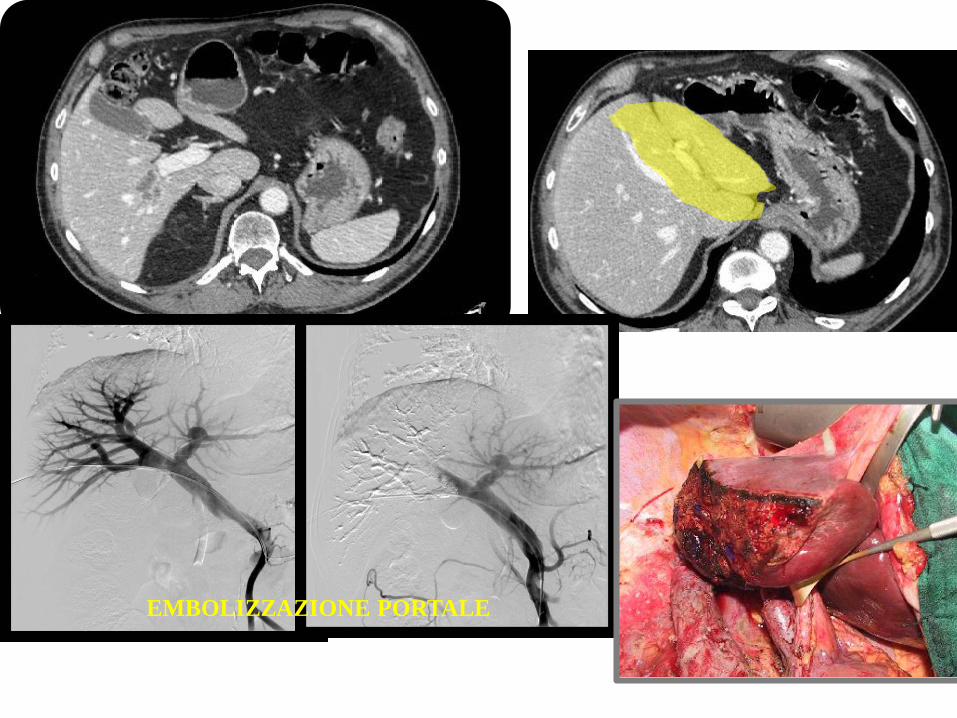
EMBOLIZZAZIONE PORTALE
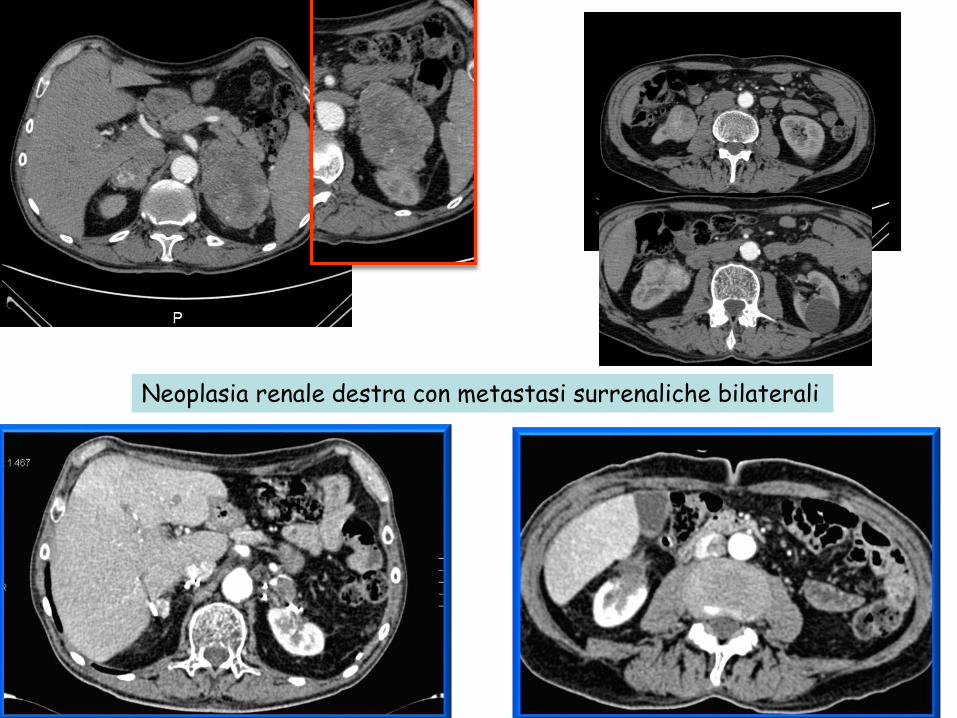
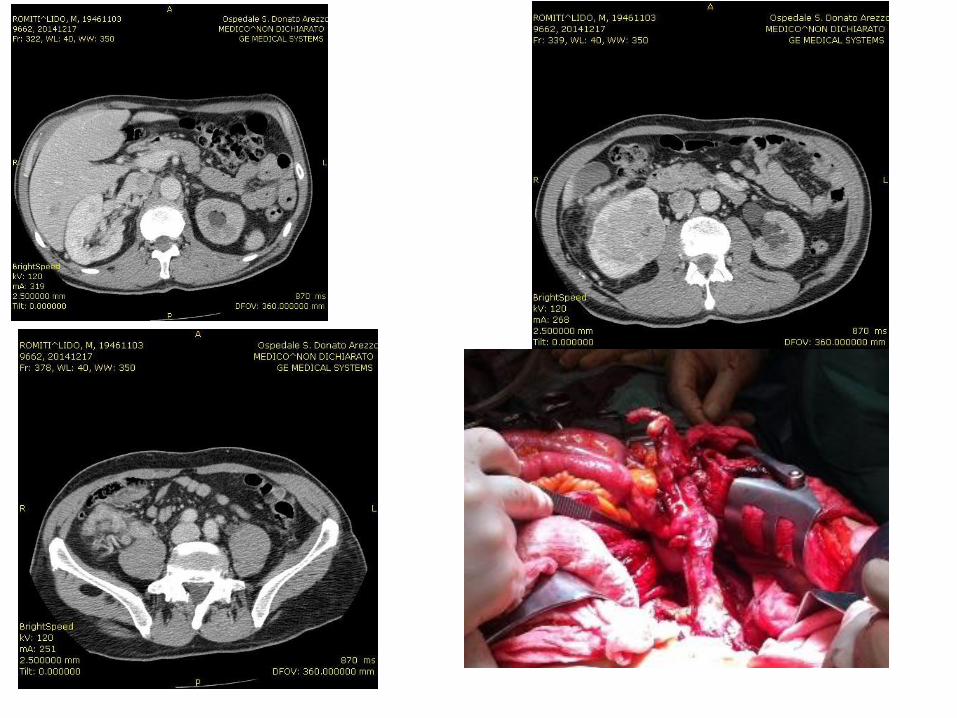
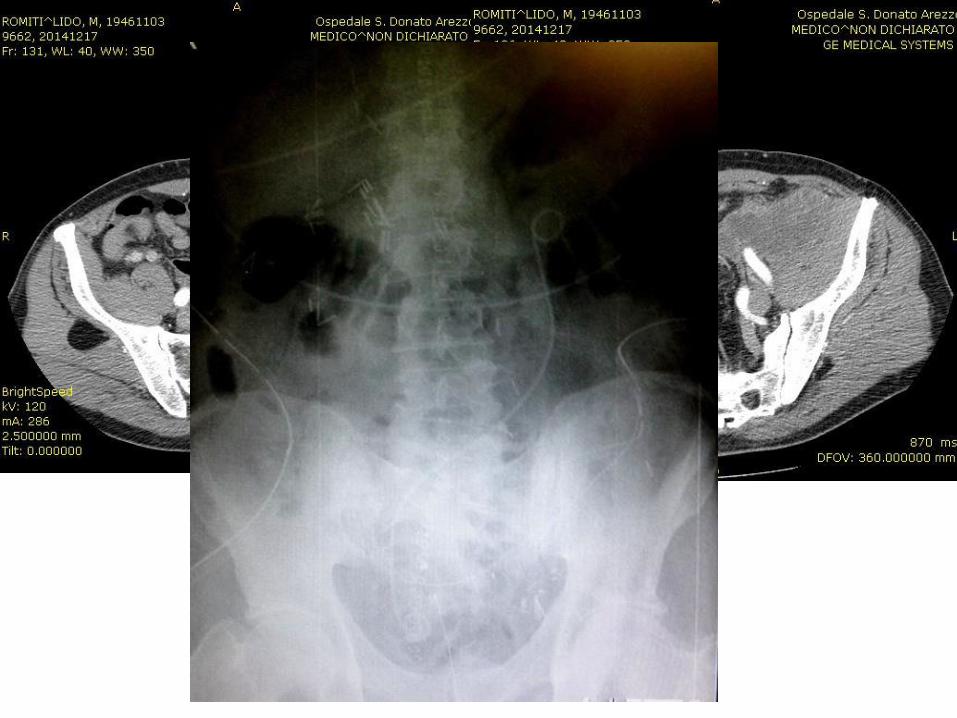
Neoplasia renale destra con metastasi surrenaliche bilaterali
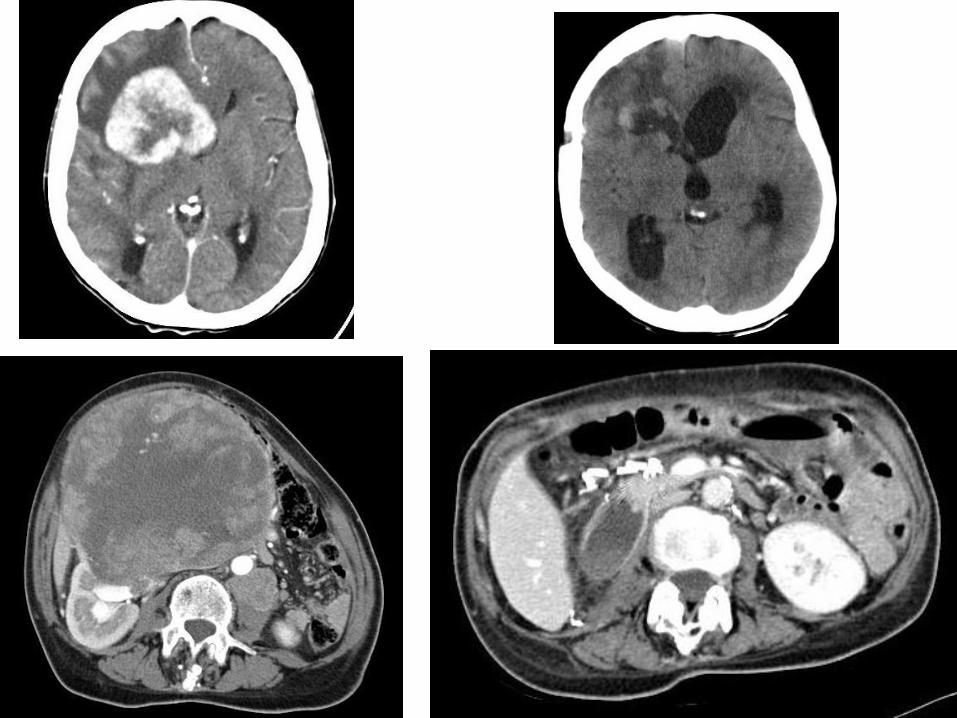

Tumore renale destro con trombosi cavale a partenza dalla vena gonadica interessata per via retrograda da collaterale polare inferiore
Voluminosa massa a sede pelvica sinistra coinvolgente uretere e grossi vasi ( metastasi atipica???)
Kidney Tumors
Bone metastasesTreatment
Prostate(32%), breast (22%), kidney (16%),lung and thyroid cancer have a high risk for metastatic bone disease. In fact, these primary carcinomas account for 80% of all the metastases to the bone
Aim of orthopedic surgery
Achieve adequate pain control Prevent or stabilize pathological fracturesPrevent spinal cord compressionIn selected cases, complete resection may improve the survival rate of the patient.

Kidney Tumors
Bone metastasesTreatment
Multidisciplinary team
Orthopaedic surgeonRadiologistRadiotherapistUrologistOncologist
There is no strict rationale governing the surgical management of skeletal metastases. Clinical, medical, radiological and surgical factors, coupled with the inherent biology of the primary tumor all contribute to the decison making process. Furthermore data about patient survival and quality of life are required

Linee Guida Trattamento Metastasi Ossee
Società Italiana di Ortopedia e Traumatologia

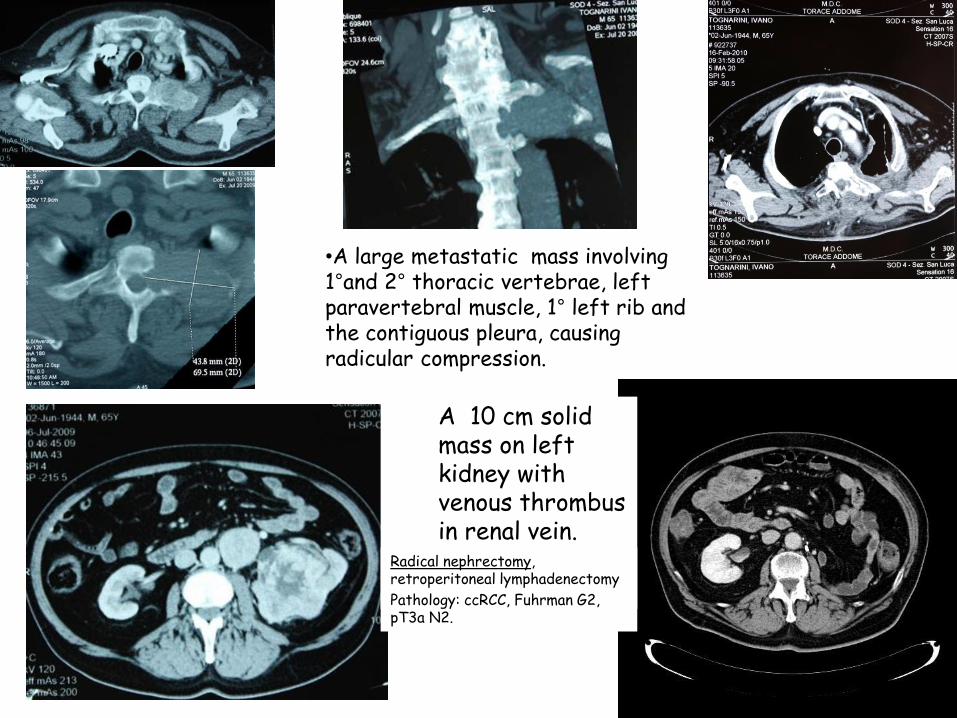
•A large metastatic mass involving 1°and 2° thoracic vertebrae, left paravertebral muscle, 1° left rib and the contiguous pleura, causing radicular compression.
A 10 cm solid mass on left kidney with venous thrombus in renal vein.
Radical nephrectomy, retroperitoneal lymphadenectomy
Pathology: ccRCC, Fuhrman G2, pT3a N2.
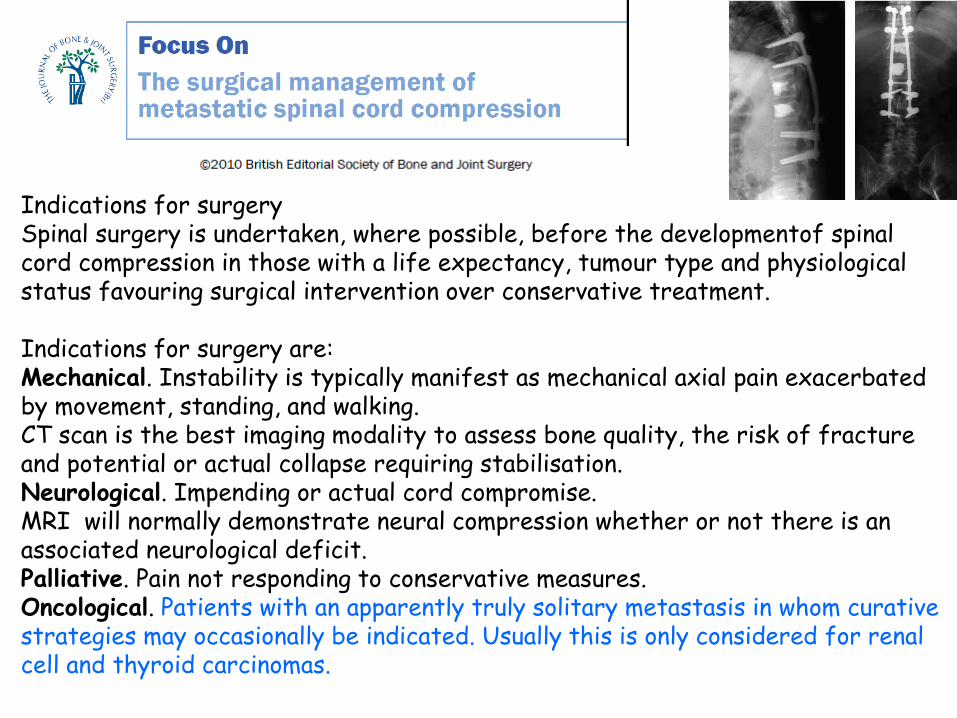
Indications for surgerySpinal surgery is undertaken, where possible, before the developmentof spinal cord compression in those with a life expectancy, tumour type and physiological status favouring surgical intervention over conservative treatment.
Indications for surgery are:Mechanical. Instability is typically manifest as mechanical axial pain exacerbated by movement, standing, and walking.CT scan is the best imaging modality to assess bone quality, the risk of fracture and potential or actual collapse requiring stabilisation.Neurological. Impending or actual cord compromise. MRI will normally demonstrate neural compression whether or not there is an associated neurological deficit.Palliative. Pain not responding to conservative measures.Oncological. Patients with an apparently truly solitary metastasis in whom curative strategies may occasionally be indicated. Usually this is only considered for renal cell and thyroid carcinomas.

proximal femur metastasis
from renal cell carcinoma
SOD Ortopedia
Oncologica
AOU Careggi
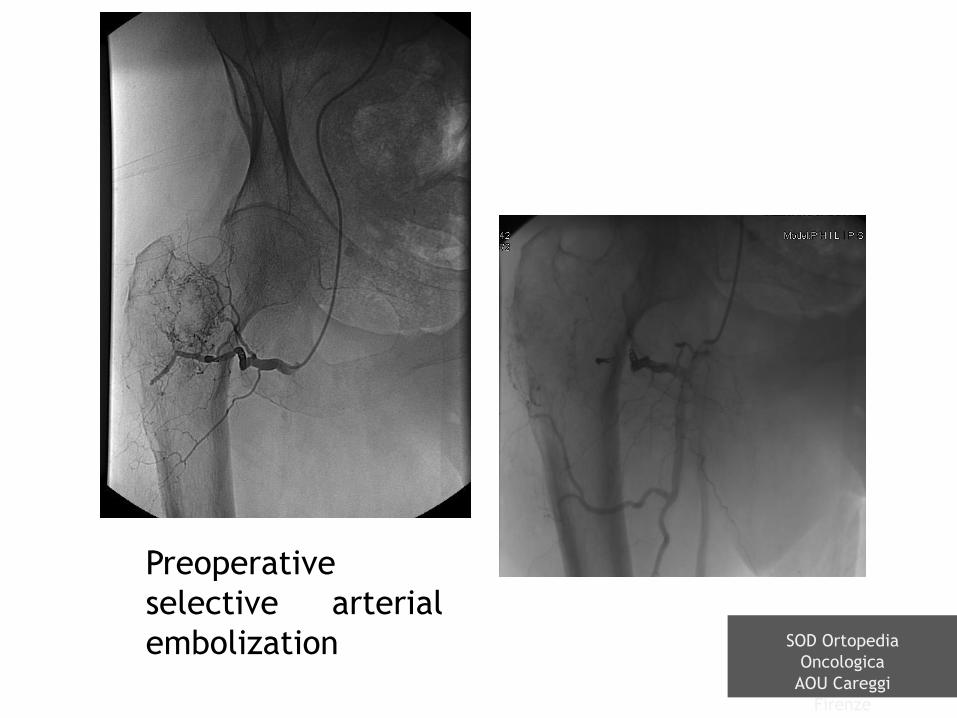
Preoperative
selective arterial
embolization SOD Ortopedia
Oncologica
AOU Careggi
Firenze

Surgical
treatment:
resection and
cemented
megaprosthesis
(with cement
reinforcing all
the canal)
SOD Ortopedia
Oncologica
AOU Careggi
Firenze
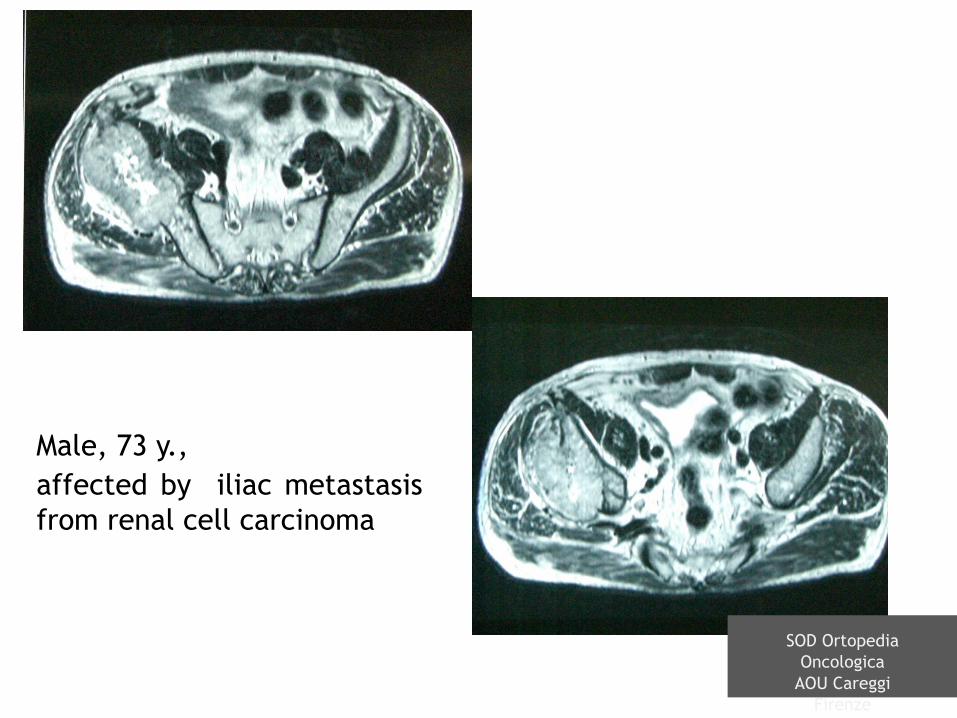
Male, 73 y.,
affected by iliac metastasis
from renal cell carcinoma
SOD Ortopedia
Oncologica
AOU Careggi
Firenze
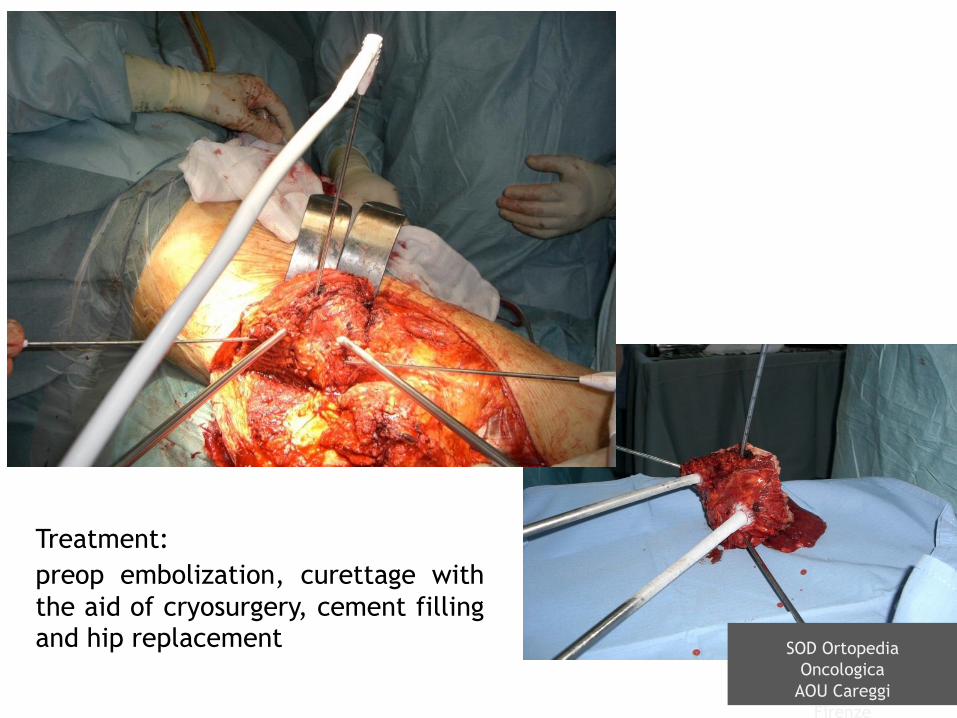
Treatment:
preop embolization, curettage with
the aid of cryosurgery, cement fillingand hip replacement SOD Ortopedia
Oncologica
AOU Careggi
Firenze
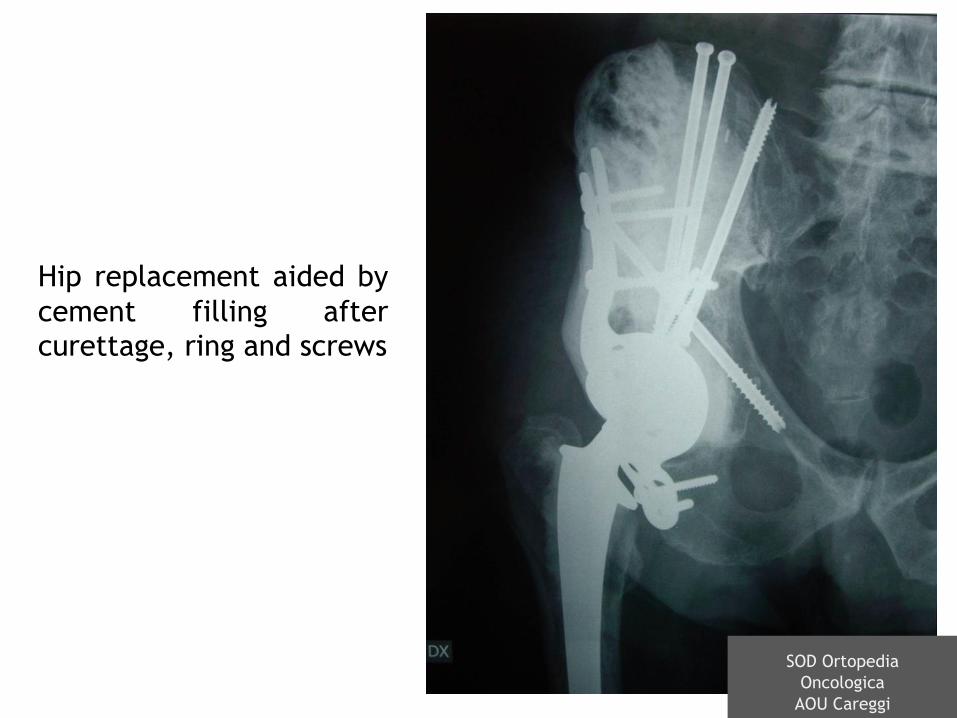
Hip replacement aided by
cement filling aftercurettage, ring and screws
SOD Ortopedia
Oncologica
AOU Careggi

Male, 57 y., left femur metastasis
SOD Ortopedia
Oncologica
AOU Careggi
Firenze
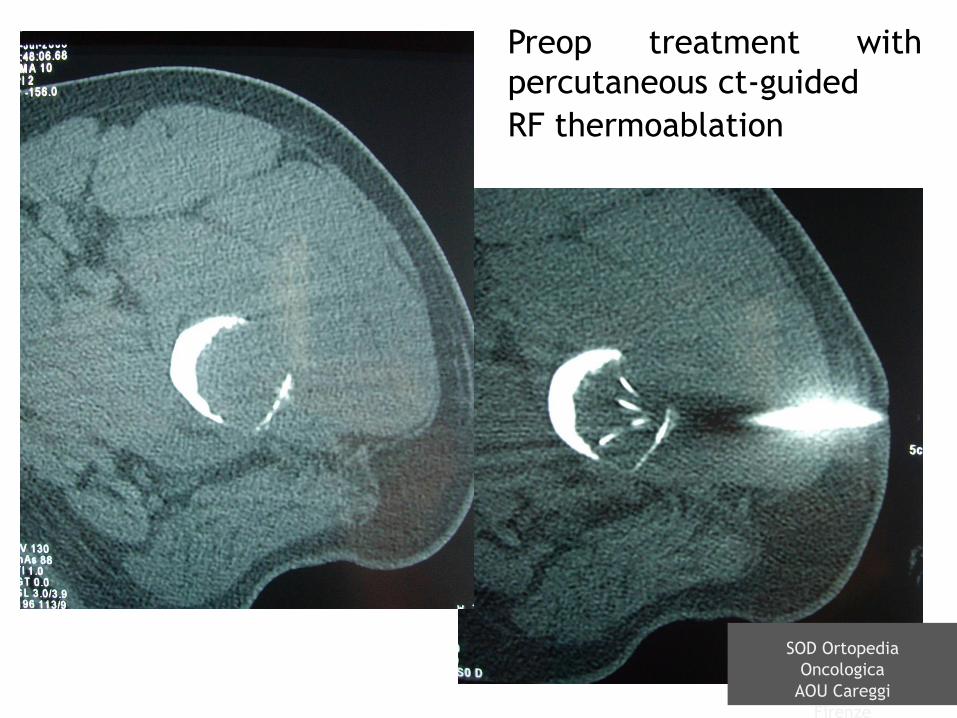
Preop treatment with
percutaneous ct-guided
RF thermoablation
SOD Ortopedia
Oncologica
AOU Careggi
Firenze

Surgical treatment:
resection and
megaprosthesis
SOD Ortopedia
Oncologica
AOU Careggi
Firenze
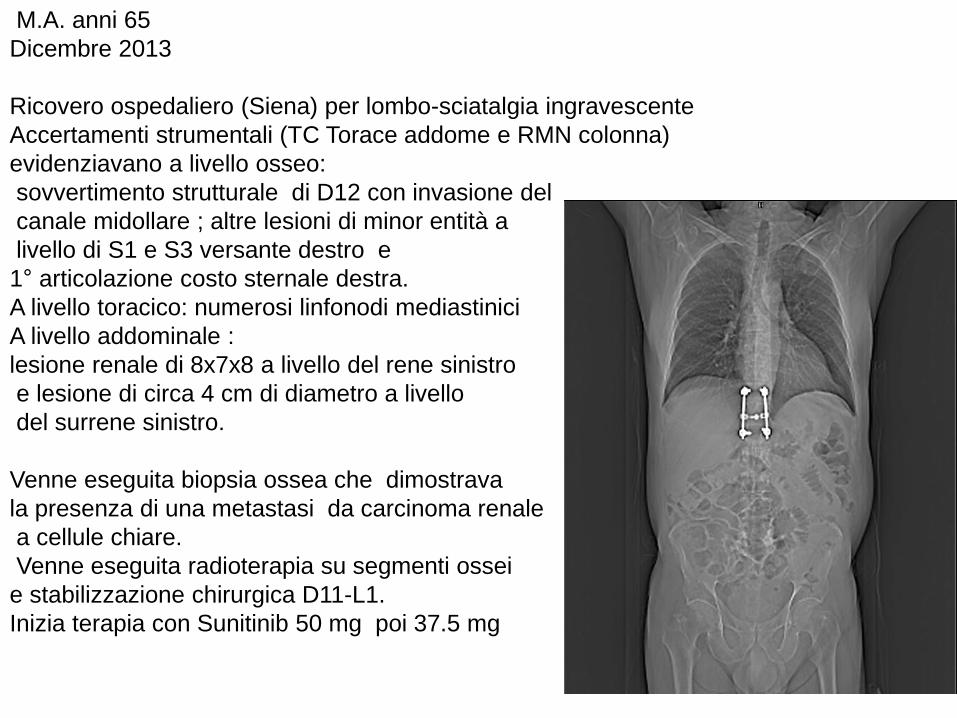
M.A. anni 65
Dicembre 2013
Ricovero ospedaliero (Siena) per lombo-sciatalgia ingravescente
Accertamenti strumentali (TC Torace addome e RMN colonna)
evidenziavano a livello osseo:
sovvertimento strutturale di D12 con invasione del
canale midollare ; altre lesioni di minor entità a
livello di S1 e S3 versante destro e
1° articolazione costo sternale destra.
A livello toracico: numerosi linfonodi mediastinici
A livello addominale :
lesione renale di 8x7x8 a livello del rene sinistro
e lesione di circa 4 cm di diametro a livello
del surrene sinistro.
Venne eseguita biopsia ossea che dimostrava
la presenza di una metastasi da carcinoma renale
a cellule chiare.
Venne eseguita radioterapia su segmenti ossei
e stabilizzazione chirurgica D11-L1.
Inizia terapia con Sunitinib 50 mg poi 37.5 mg

Ad agosto 2016 una rivalutazione clinico strumentale dimostrava la
presenza di malattia attiva solo a livello renale e surrenale sinistra.
Per tossicità interrompe terapia .
Rivalutazione a ottobre con conferma della stabilità di malattia
Gennaio 2017
Nefrectomia allargata sinistra con surrenectomia omolaterale

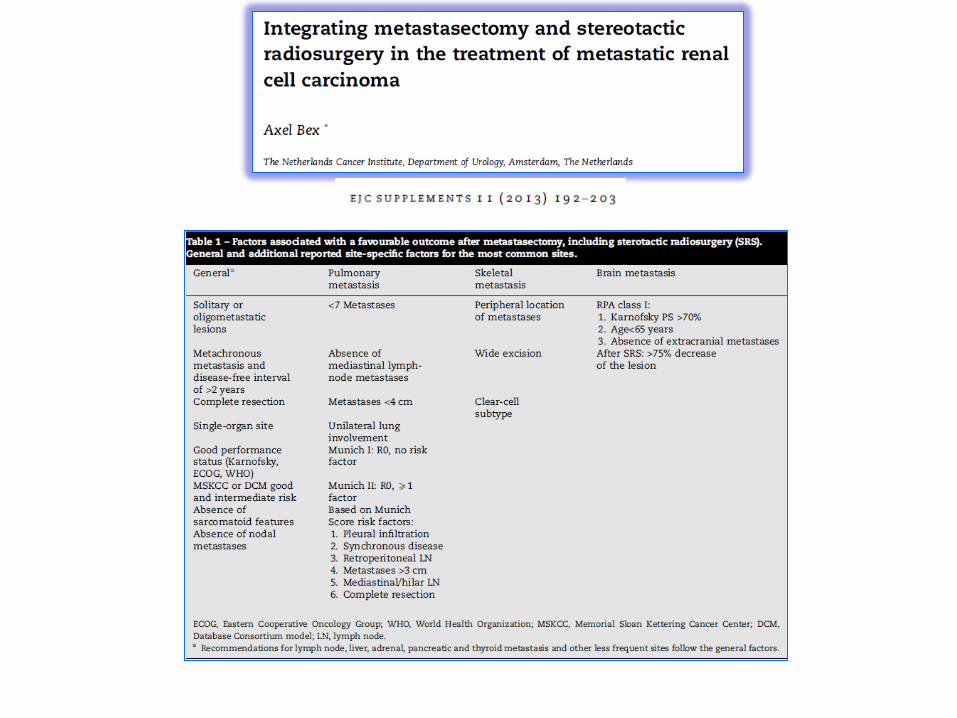
With the exception of brain and possibly bone metastases,
metastasectomy remains by default the only local treatment for
most sites.
Retrospective comparative studies consistently point towards a
benefit of complete metastasectomy in mRCC patients in terms
of overall survival, cancer-specific survival and delay of systemic
therapy.
Recommendations
No general recommendations can be made. The decision to
resect metastases has to be taken for each site, and on a
case-by-case basis; performance status, risk profiles, patient
preference and alternative techniques to achieve local control
such as stereotactic radiotherapy, must be considered.
Patients with metastatic renal cell carcinoma should be considered for multimodal therapy, including surgery of metastatic lesions. A proportion of patients will achieve long-term survival with aggressive surgical resection.







