

Introduzione

Dipartimento Malattie InfettiveASST Fatebenefratelli Sacco Hospital
Il Dipartimento di Malattie Infettive (DMI) è costituito da 2 Unità Complesse (UOC Malattie Infettive 1 * e UOC Malattie Infettive 3 clinicizzata), per un
totale di 68 posti letto accreditati (77 utilizzabili) per la degenza ordinaria, 1 Unita Semplice dipartimentale: hospice di malattie infettive con 10 posti
letto, 3 posti letto di DH e 15 postazioni per erogazione di attività ambulatoriali complesse -MAC-.
Alla UOC 1 sono assegnate l’ UOS di Allergologia e Immunologia clinica, l’UOS di Epatologia e l’UOS di Malattie Sessualmente Trasmesse.
Alla UOC III è assegnata l’ UOS di Emergenze Infettivologiche.Più di 6500 pazienti con infezione da HIV (una delle più grosse coorti di
pazienti sieropositivi d’Europa), di cui 5546 trattati nel 2016, e più di 3500 pazienti affetti da epatiti croniche di origine virale (centro accreditato da
Regione Lombardia per la prescrizione dei farmaci ad alto costo per il trattamento dell’epatite cronica C), sono seguiti costantemente presso parte
dei 18 ambulatori specialistici giornalieri afferenti al dipartimento (vedi sotto). Il DMI dell’ Ospedale Sacco è uno dei due centri di riferimento a livello
nazionale (l’altro è lo Spallanzani di Roma) per le emergenze infettivologiche (i.e patogeni infettivi di classe A che richiedono alto isolamento,
bioterrorismo), ed è stato centro di riferimento per le patologie infettive e di importazione durante Expo 2015. La ricerca e la formazione (corso di laurea
medicina e chirurgia e specializzazione e corso di laurea scienze infermieristiche) sono punti forti e qualificanti del DMI, come certificato
dall’elevato numero di pubblicazioni scientifiche internazionali prodotte (circa 50- 60 pubblicazioni indicizzate ogni anno, dipartimento con maggior impact
factor del polo universitario di competenza ).

Mission
The main mission is to provide the most technologically advanced, compassionate medical
care for our patients. We are committed to a “patients first” orientation and maintaining our well recognized excellence in patient care and
medical education.

• *1650-1700 Dimissioni/anno con oltre 9 Mi/anno ricavi
• *oltre 110000 prestazioni ambulatoriali anno con oltre 2,3 Mil/anno ricavi
• *Quasi 80 Mil file F spesi nel 2017

ResearchIn addition, we want to capture the synergies of existing and emerging opportunities
in the areas of clinical research and outcomes research to take advantage of the breadth of our clinical volume. Our research is focused mainly on HIV/AIDS (more
than 30 Phase II,III and IV trials are ongoing to date ) but our specific areas of interest range from tuberculosis through to gram positive sepsis, hospital acquired
infection, osteoarticular infections, endocarditis, travel acquired infections, etc. Some of the research programmes involve formal and informal collaboration with
colleagues at international level as well as collaboration in other university disciplines and other teaching hospitals

Who are you?
Hepatitis C virus (HCV) is a memberof the hepacivirus genus within theflaviviridae family of virus, and ithas a single positive stranded RNAmolecule (~9500 nucleotides) as itsgenome.
Although the high-resolution structure of the HCVvirion still needs to be fully elucidated, it is thought tobe around 45-100 nm in diameter and formed by anucleus of genomic RNA included in an icosahedralcapsid made of multiple copies of core protein. It islastly surrounded by a bilayer lipid membrane onwhich the viral-derived envelope glycoproteins E1and E2 are anchored (Gastaminza, J Virol 2010;Wakita Nat Med 2005).

HCV could have been coevolving with human populations during their migration out of
Africa within the past 100,000 to 150,000 years, but the current HCV genotypes
appeared much more recently.
A study suggested that types 6 and 4 could have originated 700 years and 350 years
ago, respectively, whereas subtypes 1a and 1b could have arisen less than 100
years ago.
Pybus et al Science 2001
The origin of the primate Flaviviridae could be as
ancient as the differentiation of primate species
some 35 million years ago

Viral biology
Budding
Endocytosis and uncoating
Translation and proteolyticcleavage
Replication
Assembly
Release
Recognition and entry
HCV(in hepatocytes)3
Core protein
RNARNA
Viral mRNAs RNA
pregenome Polymerase
- DNA
+/-DNA
ER/Golgi
HBV(in hepatocytes)2
Entry
Uncoating and trafficking
cccDNAformation
Endosome
Secretion
HBsAg
1. De Clercq E. Nat Rev Drug Discov 2002;1(1):13-25. 2. Zoulim F, et al. Antiviral Res 2012;96(2):256-9. 3. Schaefer E, Chung R. Gastroenterology 2012;142(6):1340-50. Covalently closed-circular HBV DNA, cccDNA
Viral proteins and RNA assemble at cell membrane
Proteolytic processing by viral protease
Translation
Transcription
Integration
Reverse transcription
Uncoating
DNA
Virus–cell fusion
Virus adsorption
Envelope
Receptor and co-receptor proteins
Capsid coreReverse transcriptase
RNA
HIV(in CD4)1
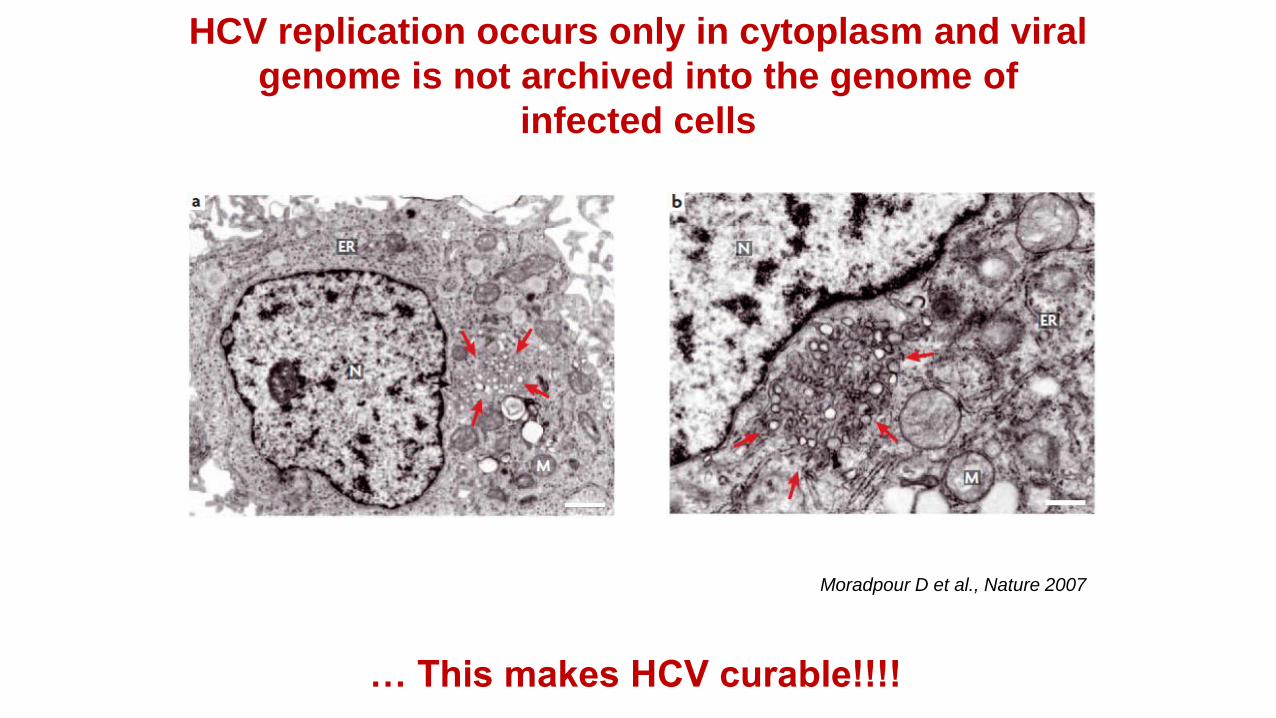
Moradpour D et al., Nature 2007
HCV replication occurs only in cytoplasm and viral
genome is not archived into the genome of
infected cells
… This makes HCV curable!!!!
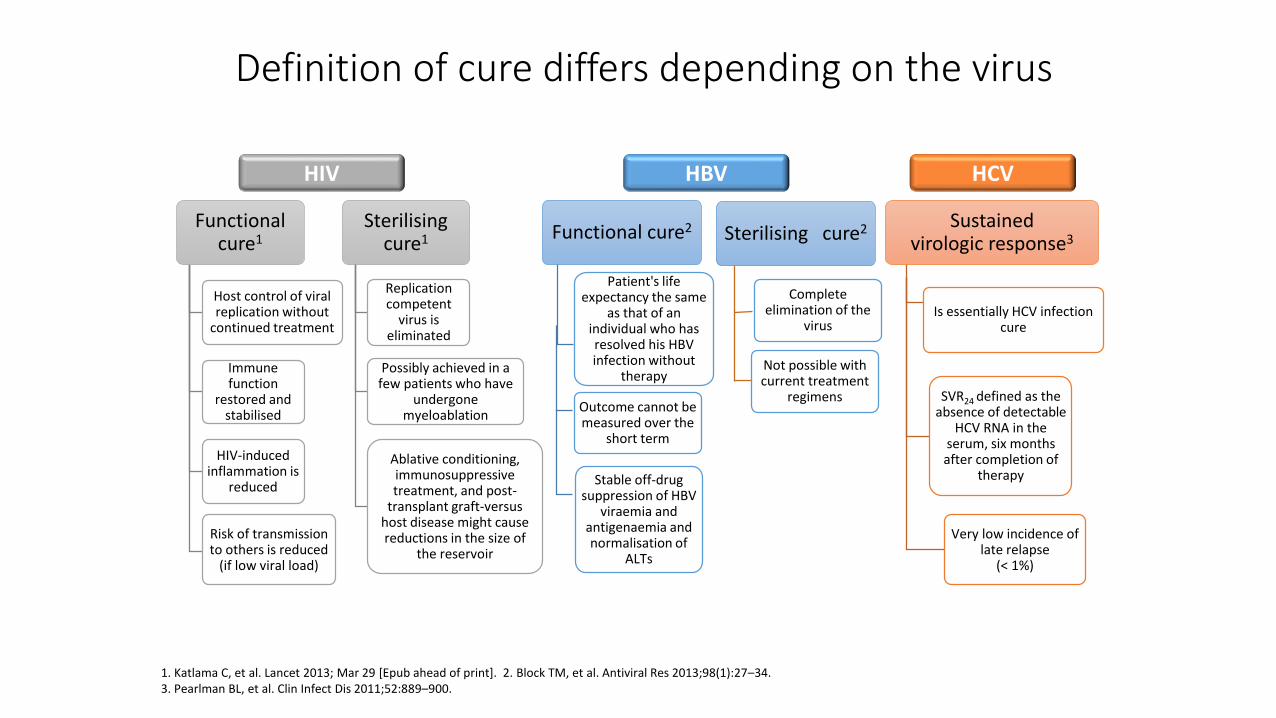
Definition of cure differs depending on the virus
1. Katlama C, et al. Lancet 2013; Mar 29 [Epub ahead of print]. 2. Block TM, et al. Antiviral Res 2013;98(1):27–34. 3. Pearlman BL, et al. Clin Infect Dis 2011;52:889–900.
Host control of viral replication without
continued treatment
Immune function
restored and stabilised
HIV-induced inflammation is
reduced
Risk of transmission to others is reduced
(if low viral load)
Functional cure1
Replication competent
virus is eliminated
Possibly achieved in a few patients who have
undergone myeloablation
Ablative conditioning, immunosuppressive treatment, and post-
transplant graft-versus host disease might cause reductions in the size of
the reservoir
Sterilising cure1
HIV HBV
Is essentially HCV infection cure
SVR24 defined as the absence of detectable
HCV RNA in the serum, six months after completion of
therapy
Very low incidence of late relapse
(< 1%)
Sustained virologic response3
HCV
Sterilising cure2
Complete elimination of the
virus
Not possible with current treatment
regimens
Patient's life expectancy the same
as that of an individual who has resolved his HBV infection without
therapy
Outcome cannot be measured over the
short term
Functional cure2
Stable off-drug suppression of HBV
viraemia and antigenaemia and normalisation of
ALTs

Hepatitis C: 25 years since discovery
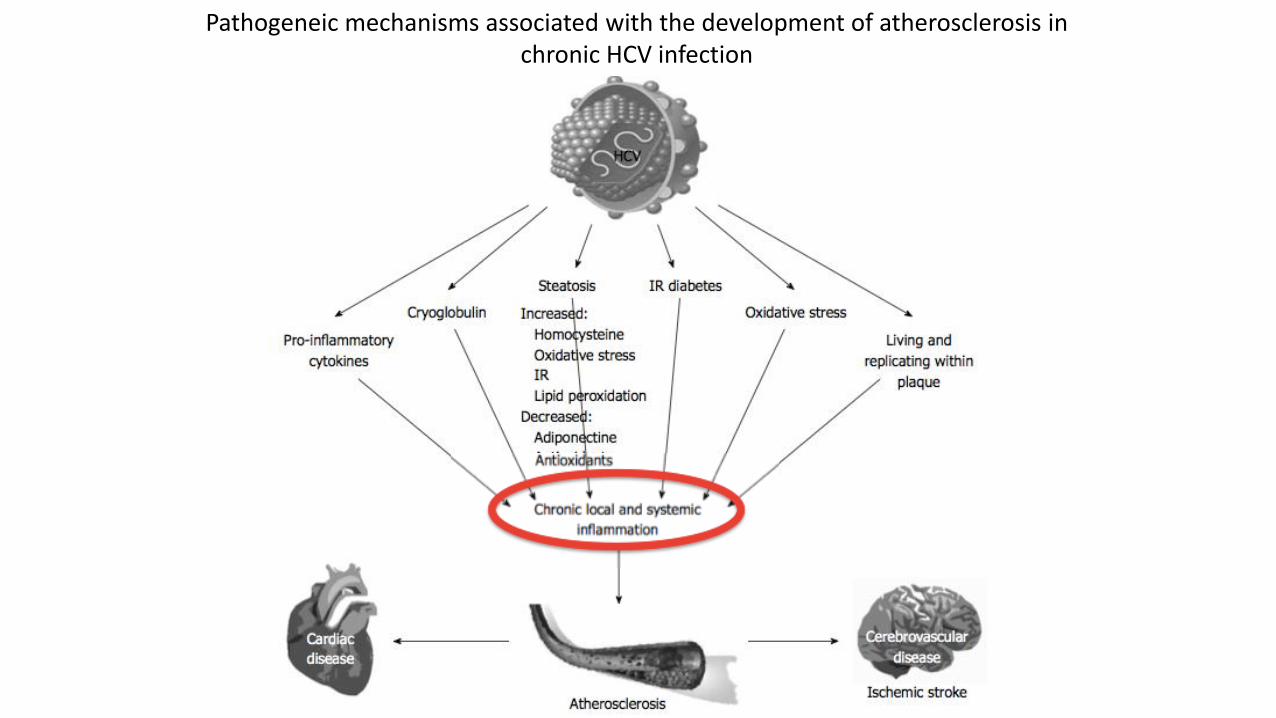
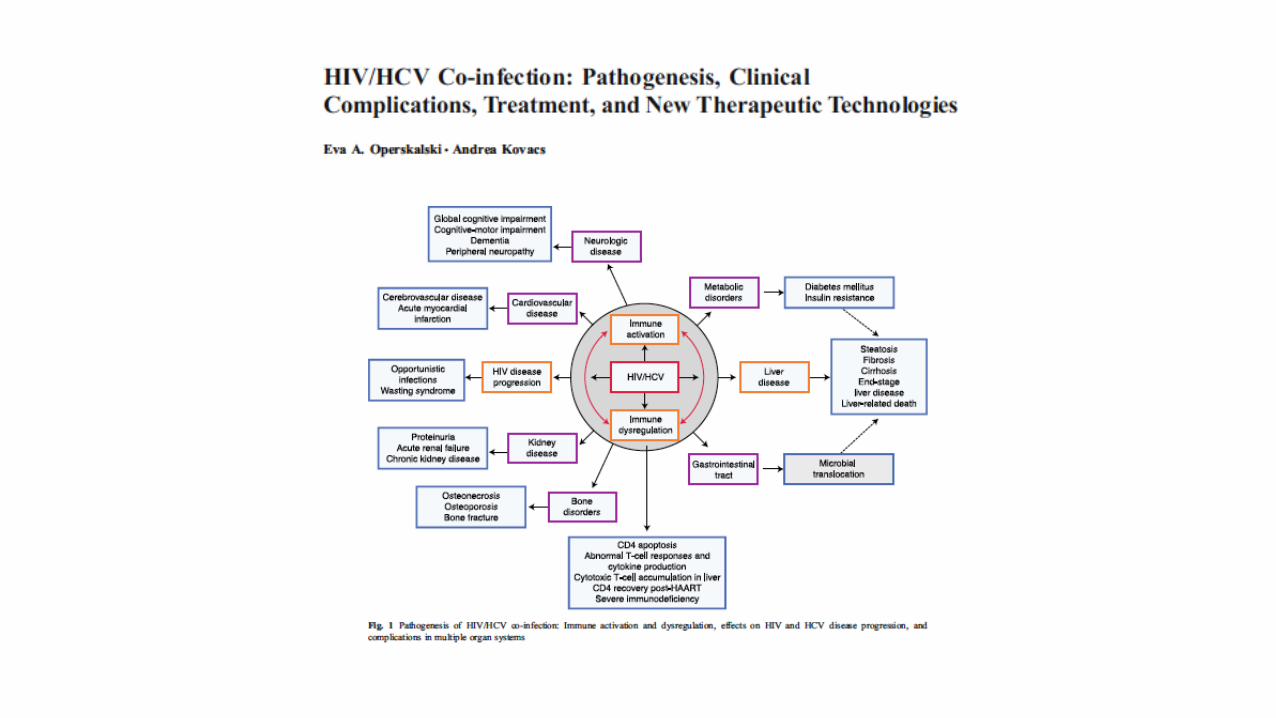
Pathogeneic mechanisms associated with the development of atherosclerosis in chronic HCV infection
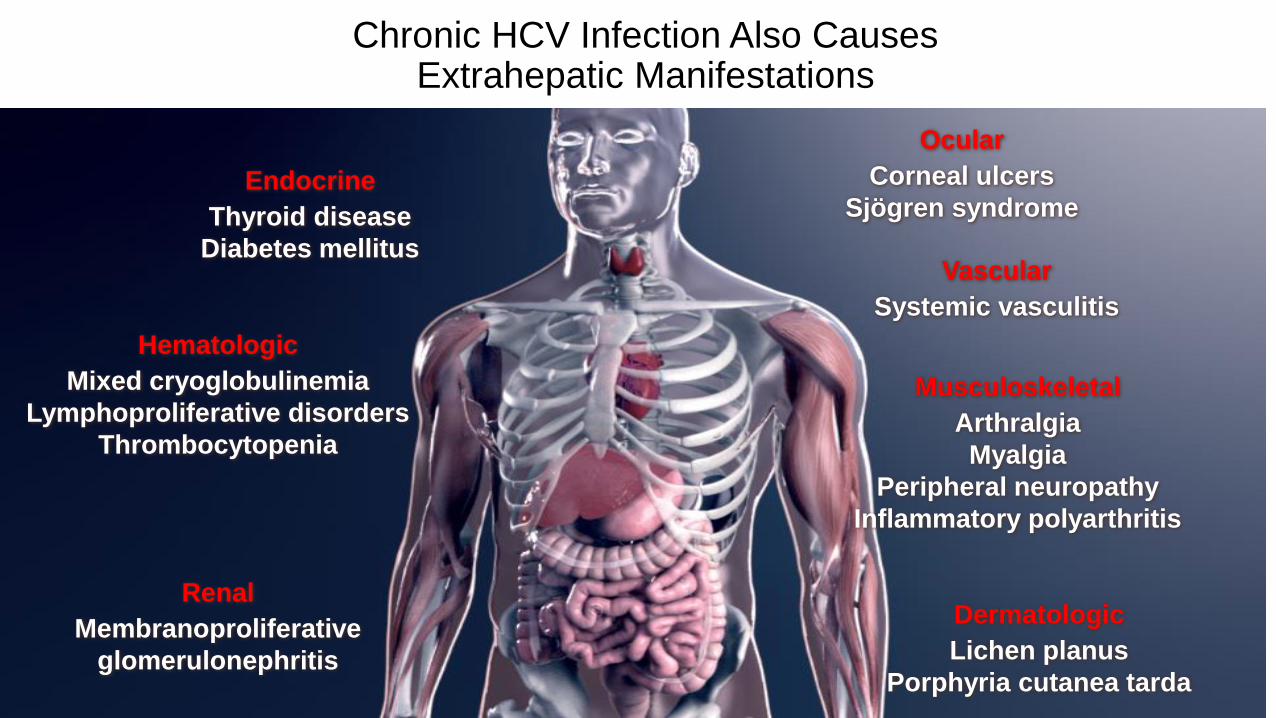
Chronic HCV Infection Also Causes Extrahepatic Manifestations
Endocrine
Thyroid disease
Diabetes mellitus
Hematologic
Mixed cryoglobulinemia
Lymphoproliferative disorders
Thrombocytopenia
Renal
Membranoproliferative
glomerulonephritis
Ocular
Corneal ulcers
Sjögren syndrome
Vascular
Systemic vasculitis
Dermatologic
Lichen planus
Porphyria cutanea tarda
Musculoskeletal
Arthralgia
Myalgia
Peripheral neuropathy
Inflammatory polyarthritis

Co-morbidities in HCV patients are relevant – bringing potential for competing risks
Vutien P, et al. AASLD 2014; Poster #1481.
Depression
Atherosclerosis Lymphoma
Substance
misuse
Diabetes
Renal disease
Cognitive
impairmentPsychosis
Respiratory
disease
Dyslipidaemia
Cardiovascular
disease
Cancer HIV
co-infection
92% HCV patients
had co-morbidities
40% had 5 or more
co-morbidities

*Includes persons from CHeCS and SEER ages 25 and older. Includes 565 incident cancers in 543 patients; 22 second cancers were histologically distinct from first. Includes all SEER 13 registries except Alaska Natives. §Tobacco-related cancer. ||Alcohol-related cancer.
Journal of Hepatology 2015


• La gestione corrente dell’infezione cronica da HCV:
dati real-world

Real-wold data
•Perchè sono utili e quali ne sono i limiti

Observational vs randomized studies: Differences
• Randomized: • Treated/untreated groups more likely to be
comparable;• Treatment regimen and outcome assessment more
certain;• Risk factor, adherence info often better.
• Observational:• Subjects often more representative;• Usage conditions usually more typical;• Larger size/ longer duration possibilities permit
observation of rare / delayed outcomes.
Why perform observational studies?
• Understand experiences of actual users under conditions of actual use – nearly always different from clinical trials.
• Provide timely information by assessing accumulated experience.
• Assess very large populations.
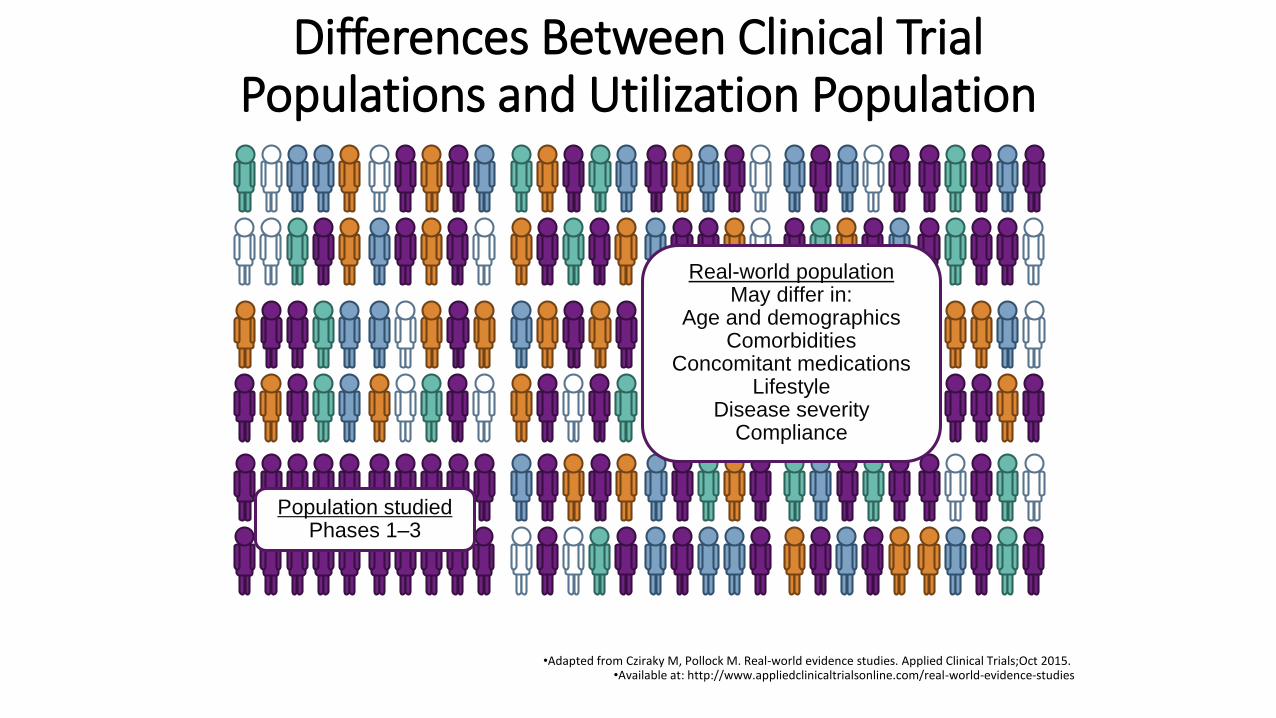
Differences Between Clinical Trial Populations and Utilization Population
•Adapted from Cziraky M, Pollock M. Real-world evidence studies. Applied Clinical Trials;Oct 2015. •Available at: http://www.appliedclinicaltrialsonline.com/real-world-evidence-studies
Real-world populationMay differ in:
Age and demographicsComorbidities
Concomitant medicationsLifestyle
Disease severityCompliance
Population studiedPhases 1–3

High Rates of SVR in HCV GT1 Mono-Infected Patients in Clinical Trials
•* Not including patients with GT1a and baseline NS5A polymorphisms; testing is recommended for patients with GT1a infection; † Based on limited data.
•Zepatier US Prescribing Information (accessed May 2016);Viekirax & Exviera, Harvoni, Olysio, and Daklinza
•Summary of Product Characteristics (all accessed May 2016).
SVR90–100%
SVR87–100%
SVR90–100%
SVR98–100%
SVR94*–100%
OBV/PTV/r +
DSV ± RBV
EBR/GZR ± RBV
DCV + SOF
± RBV†
SMV + SOF
± RBV
LDV/SOF± RBV
High SVR12 rates in
GT1-infected patients in
clinical trials

•* Not including patients with GT1a and baseline NS5A polymorphisms; testing is recommended for patients with GT1a infection; † Based on limited data.
•Zepatier US Prescribing Information (accessed May 2016);Viekirax & Exviera, Harvoni, Olysio, and Daklinza
•Summary of Product Characteristics (all accessed May 2016).
SVR90–100%
SVR87–100%
SVR90–100%
SVR98–100%
SVR94*–100%
OBV/PTV/r +
DSV ± RBV
EBR/GZR ± RBV
DCV + SOF
± RBV†
SMV + SOF
± RBV
LDV/SOF± RBV
Are we replicating this in the real world?
?

Real-world
• Confronto tra diversi regimi di trattamento in real life• Dati real life e studi clinici
• Coinfezione HIV-HCV in real life• Il cirrotico scompensato
• Real-Italia• Real-Lombardia• Real-Sacco

Real-world
• Confronto tra diversi regimi di trattamento in real life• Dati real life e studi clinici
• Coinfezione HIV-HCV in real life• Il cirrotico scompensato
• Real-Italia• Real-Lombardia• Real-Sacco

• HCV-TARGET is a consortium of academic (n=39) and community (n=13) medical centers in the U.S., Germany, Israel and Canada conducting a longitudinal, observational study
• HCV treatment is administered according to local standard of care, and regimen selection is made by the patient’s health care provider
• Data from sequentially enrolled patients undergoing HCV therapy is captured from medical records within a common database utilizing novel, centralized data abstraction
• Demographic, clinical, adverse event, and virologic data is collected through treatment and follow-up
Methods

Terrault N et al AASLD 2015

Safety and Effectiveness of DAA Regimens in Kidney and/or Liver Transplant Recipients with HCV
Reddy, EASL 2016, Poster Sat-189 29
HCV-TARGET
Kidney
Transplant
N=31
Liver
Transplant
N=229
Kidney/Liver
Transplant
N=23
Total
N=283
Male, n (%) 19 (61.3) 173 (75.5) 18 (78.3) 210 (74.2)
Age 65+, n (%) 5 (16.1) 68 (29.7) 12 (52.2) 85 (30.0)
White, n (%) 14 (45.2) 178 (77.7) 13 (56.5) 205 (72.4)
Black, n (%) 10 (32.3) 18 (7.9) 4 (17.4) 32 (11.3)
GT, %
1a / 1b 51.6 / 32.3 58.1 / 26.6 56.5 / 34.8 57.2 / 27.9
TE, n (%) 10 (32.3) 136 (59.4) 13 (56.5) 159 (56.2)
Cirrhosis, n (%) 10 (32.3) 107 (46.7) 11 (47.8) 128 (45.2)
Treatment regimen, n
LDV/SOF±RBV
OBV/PTV/RTV/DSV±RBV
DCV+SOF±RBV
27
4
0
222
4
3
21
2
0
270 (95)
10 (4)
3 (1)
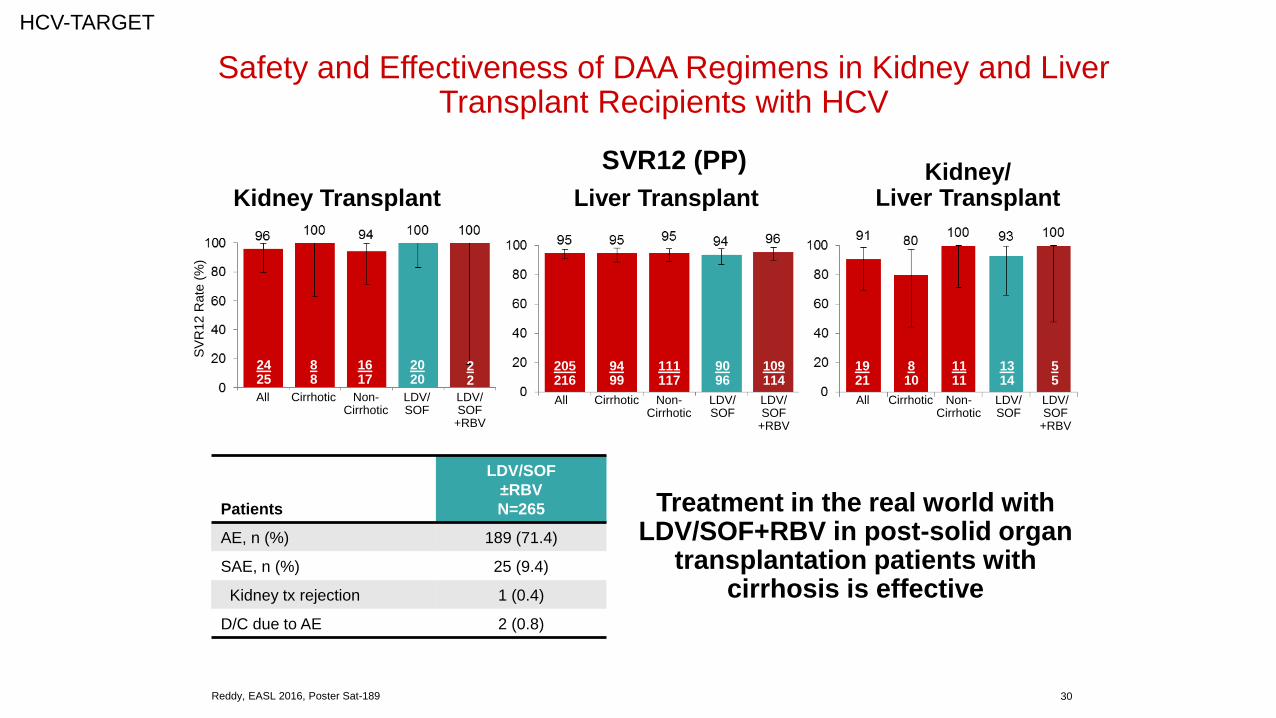
Safety and Effectiveness of DAA Regimens in Kidney and Liver Transplant Recipients with HCV
Reddy, EASL 2016, Poster Sat-189 30
HCV-TARGET
SVR12 (PP)
Kidney Transplant Liver TransplantKidney/
Liver Transplant
Patients
LDV/SOF
±RBV
N=265
AE, n (%) 189 (71.4)
SAE, n (%) 25 (9.4)
Kidney tx rejection 1 (0.4)
D/C due to AE 2 (0.8)
SV
R12 R
ate
(%
)
2425
88
1617
2020
205216
9499
111117
9096
109114
1921
810
1111
1314
55
Treatment in the real world with LDV/SOF+RBV in post-solid organ
transplantation patients with cirrhosis is effective
All Cirrhotic Non-Cirrhotic
LDV/SOF
LDV/SOF
+RBV
All Cirrhotic Non-Cirrhotic
LDV/SOF
LDV/SOF
+RBV
All Cirrhotic Non-Cirrhotic
LDV/SOF
LDV/SOF
+RBV
22







