38
NAFLD E SINDROME METABOLICA Raffaele IORIO Settore di Epatologia Dipartimento di Pediatria Università di Napoli Federico II

NAFLD E SINDROME METABOLICA
Raffaele IORIO
Settore di Epatologia
Dipartimento di Pediatria
Università di Napoli Federico II
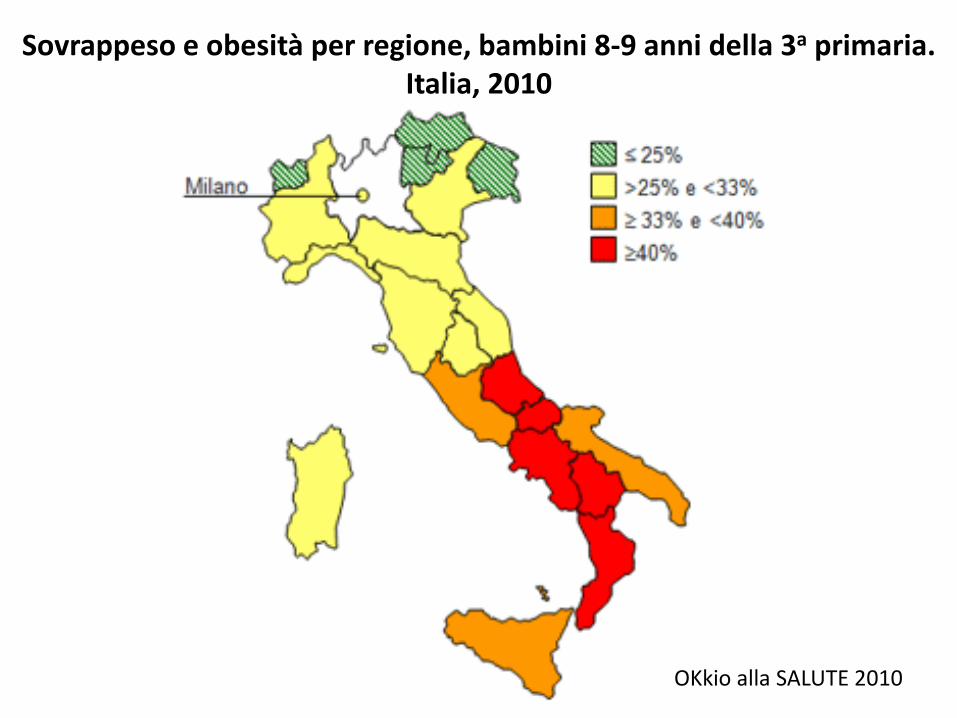
Sovrappeso e obesità per regione, bambini 8-9 anni della 3a primaria. Italia, 2010
OKkio alla SALUTE 2010

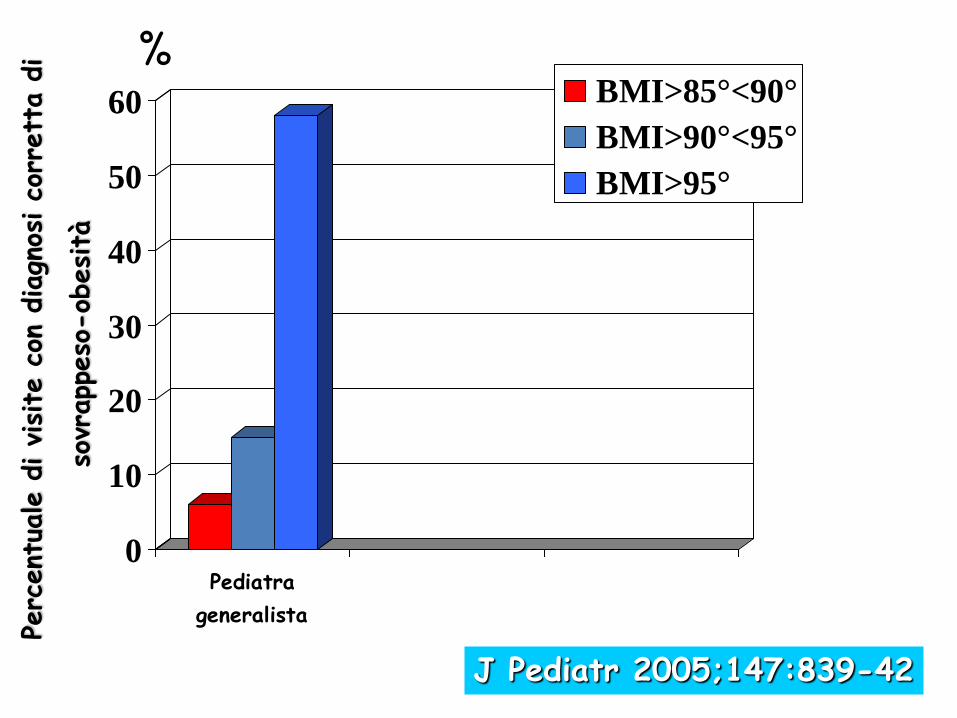
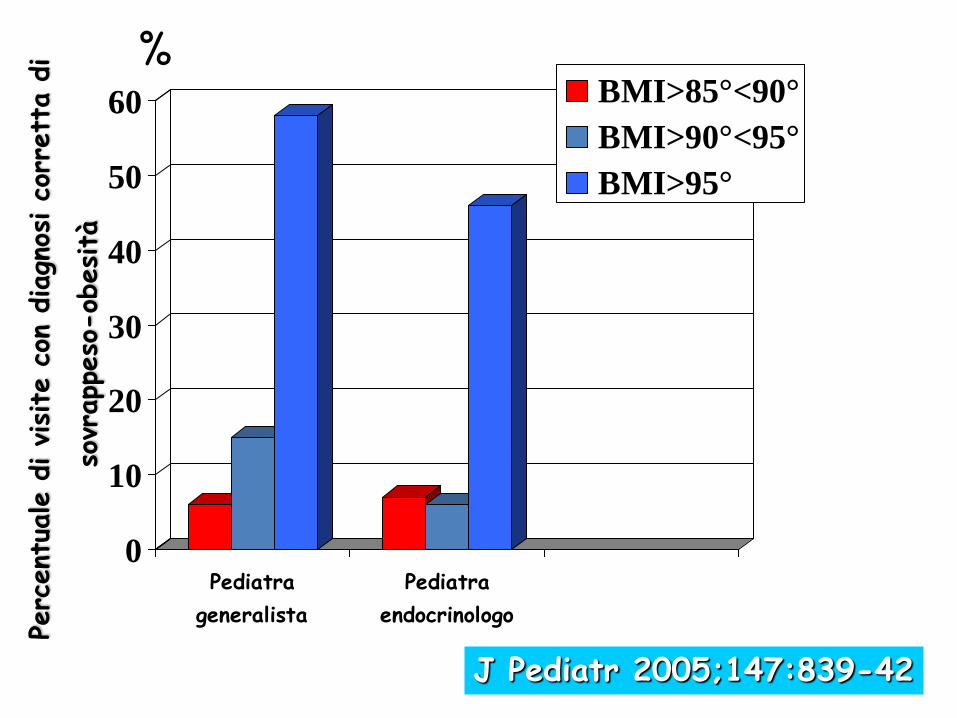
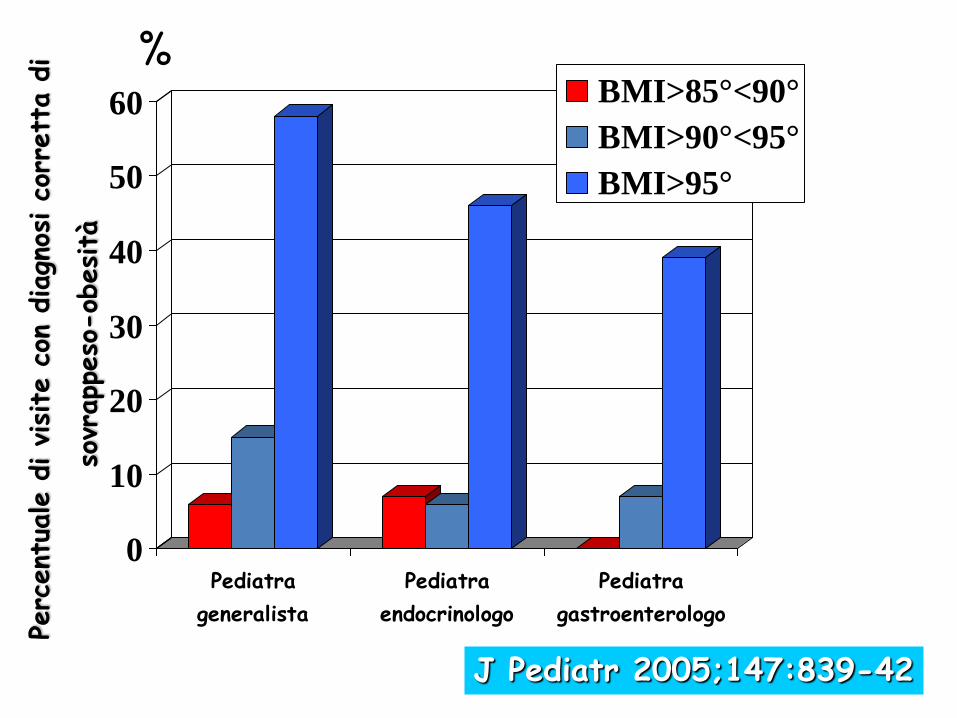
La diagnosi di obesità e fegato grasso dipende dal pediatra che
ti visita?
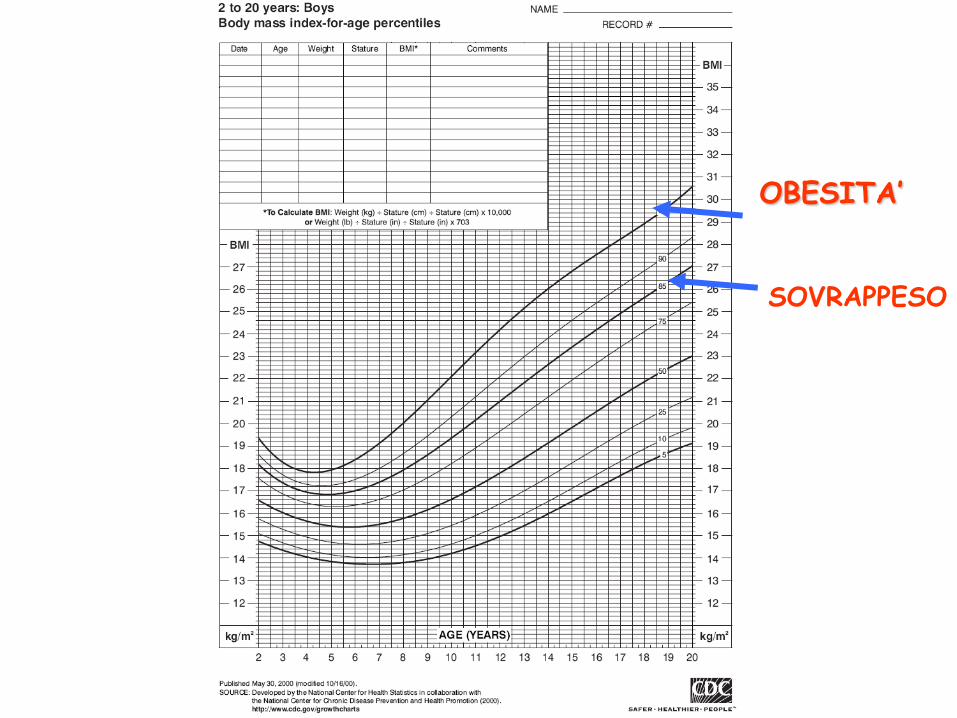
SOVRAPPESO
OBESITA’
0
10
20
30
40
50
60
Pediatra
generalista
BMI>85°<90°
BMI>90°<95°
BMI>95°
% Pe
rcent
uale d
i visite
con
diagn
osi co
rrett
a d
i
sov
rapp
eso
-ob
esità
J Pediatr 2005;147:839-42
0
10
20
30
40
50
60
Pediatra
generalista
Pediatra
endocrinologo
BMI>85°<90°
BMI>90°<95°
BMI>95°
% Pe
rcent
uale d
i visite
con
diagn
osi co
rrett
a d
i
sov
rapp
eso
-ob
esità
J Pediatr 2005;147:839-42
0
10
20
30
40
50
60
Pediatra
generalista
Pediatra
endocrinologo
Pediatra
gastroenterologo
BMI>85°<90°
BMI>90°<95°
BMI>95°
% Pe
rcent
uale d
i visite
con
diagn
osi co
rrett
a d
i
sov
rapp
eso
-ob
esità
J Pediatr 2005;147:839-42
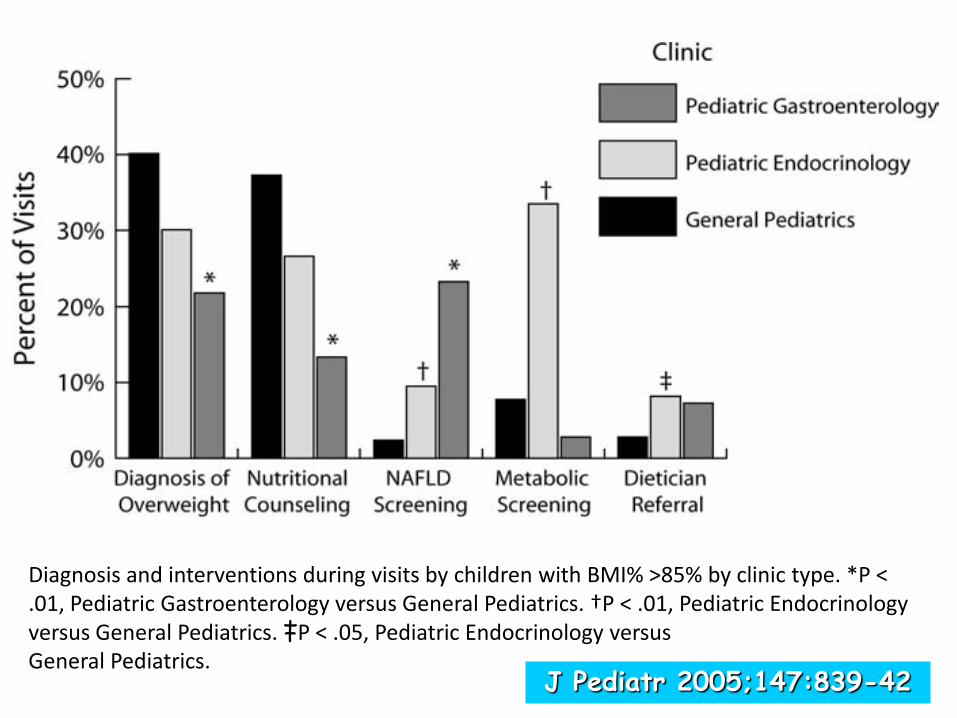
Diagnosis and interventions during visits by children with BMI% >85% by clinic type. *P < .01, Pediatric Gastroenterology versus General Pediatrics. †P < .01, Pediatric Endocrinology versus General Pediatrics. ‡P < .05, Pediatric Endocrinology versus General Pediatrics.
J Pediatr 2005;147:839-42
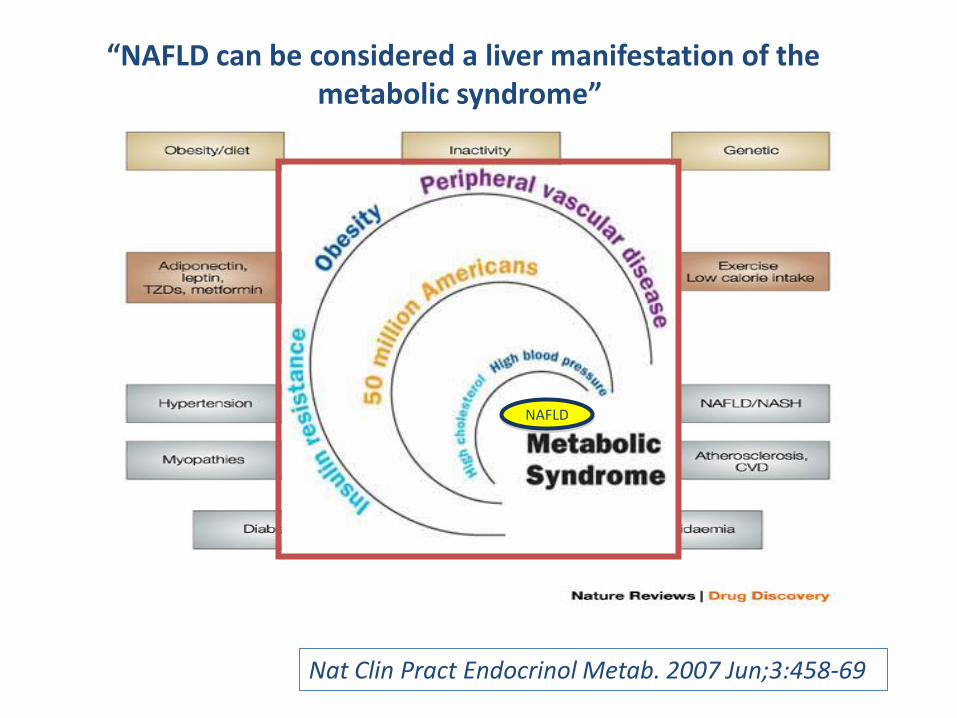
Nat Clin Pract Endocrinol Metab. 2007 Jun;3:458-69
“NAFLD can be considered a liver manifestation of the metabolic syndrome”
NAFLD
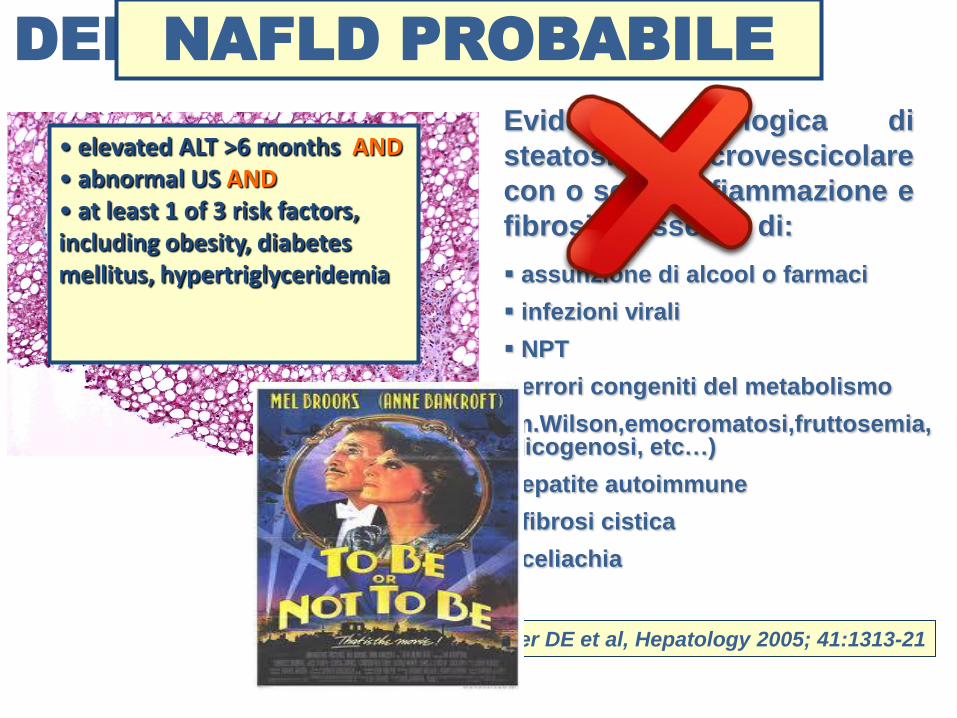
DEFINIZIONE DI NAFLD
assunzione di alcool o farmaci
infezioni virali
NPT
errori congeniti del metabolismo
(m.Wilson,emocromatosi,fruttosemia,glicogenosi, etc…)
epatite autoimmune
fibrosi cistica
celiachia
Evidenza istologica di
steatosi macrovescicolare
con o senza infiammazione e
fibrosi in assenza di:
Kleiner DE et al, Hepatology 2005; 41:1313-21
• elevated ALT >6 months AND • abnormal US AND • at least 1 of 3 risk factors, including obesity, diabetes mellitus, hypertriglyceridemia
NAFLD PROBABILE
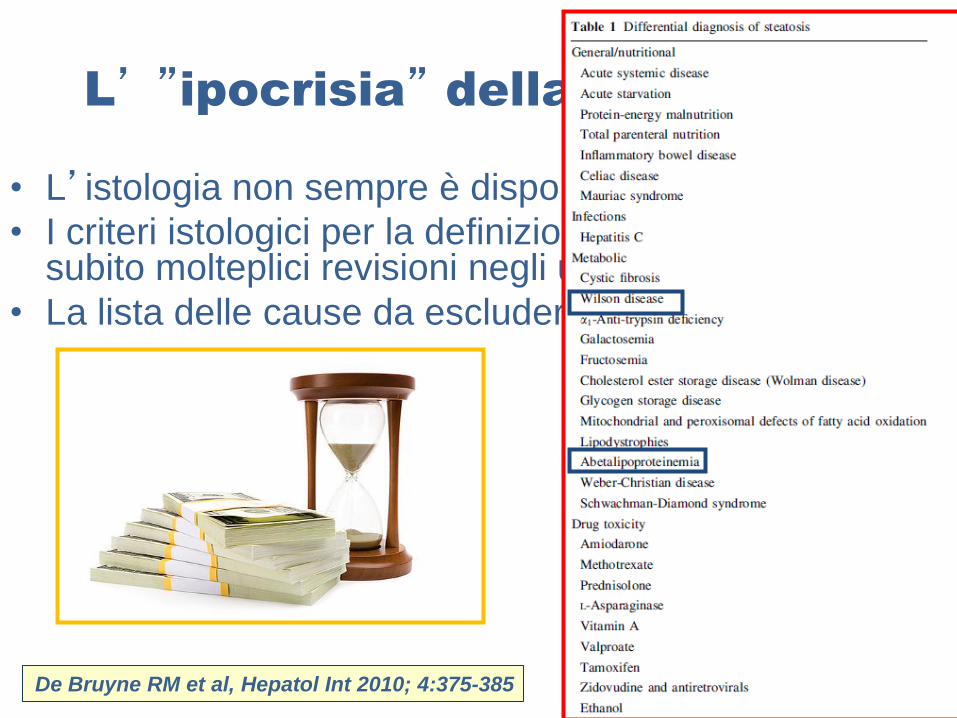
L’ ”ipocrisia” della definizione
• L’istologia non sempre è disponibile
• I criteri istologici per la definizione della NAFLD hanno subito molteplici revisioni negli ultimi anni
• La lista delle cause da escludere è lunga e complessa
De Bruyne RM et al, Hepatol Int 2010; 4:375-385
PREVALENZA DELLA NAFLD
in pediatria
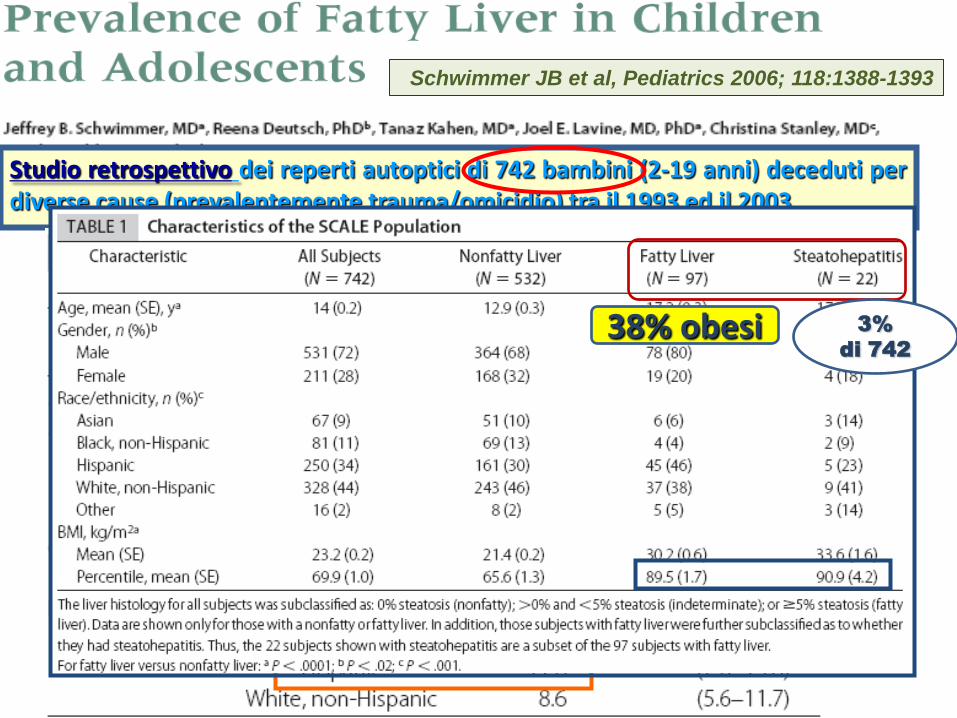
Studio retrospettivo dei reperti autoptici di 742 bambini (2-19 anni) deceduti per diverse cause (prevalentemente trauma/omicidio) tra il 1993 ed il 2003
Schwimmer JB et al, Pediatrics 2006; 118:1388-1393
Schwimmer JB et al Hepatology 2005; 42:641-648
38% obesi 3%
di 742
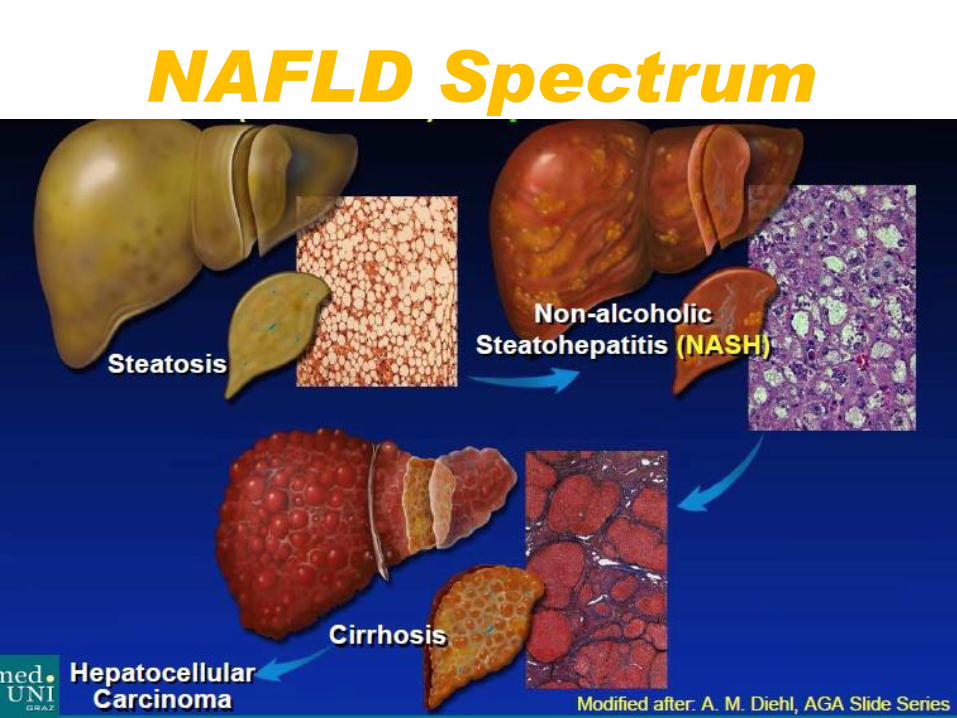
NAFLD Spectrum

La storia naturale della
NAFLD?
Priess et al, Clinical Science 2008; 115:141-150
Fassio et al, Hepatology 2004; 40:820-826
Day et al, Gastroenterology 2005; 129:375-378
ADULTI
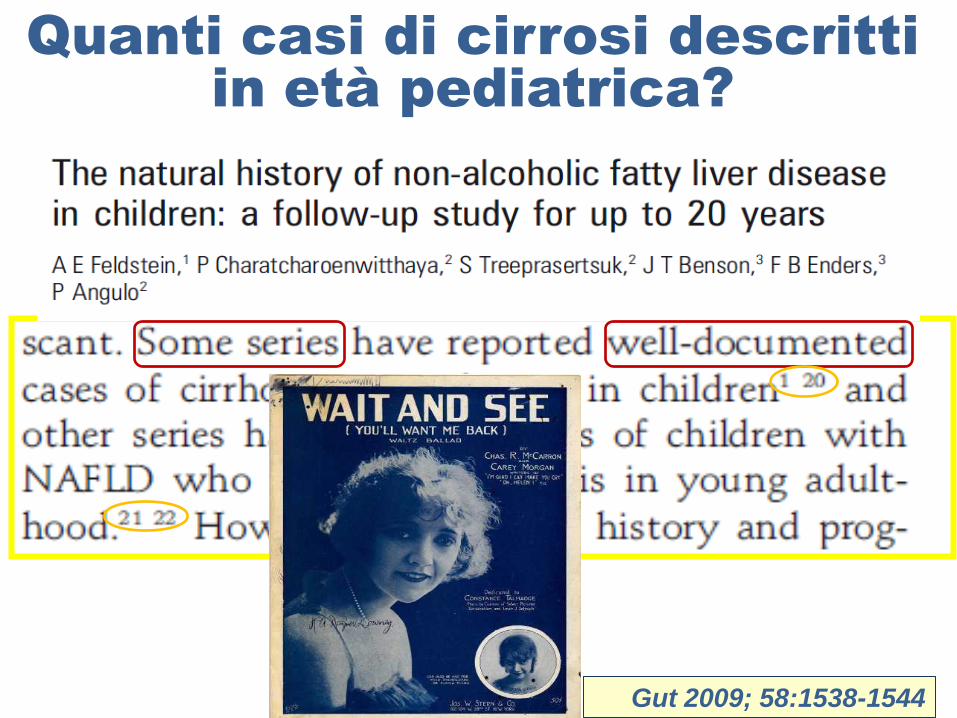
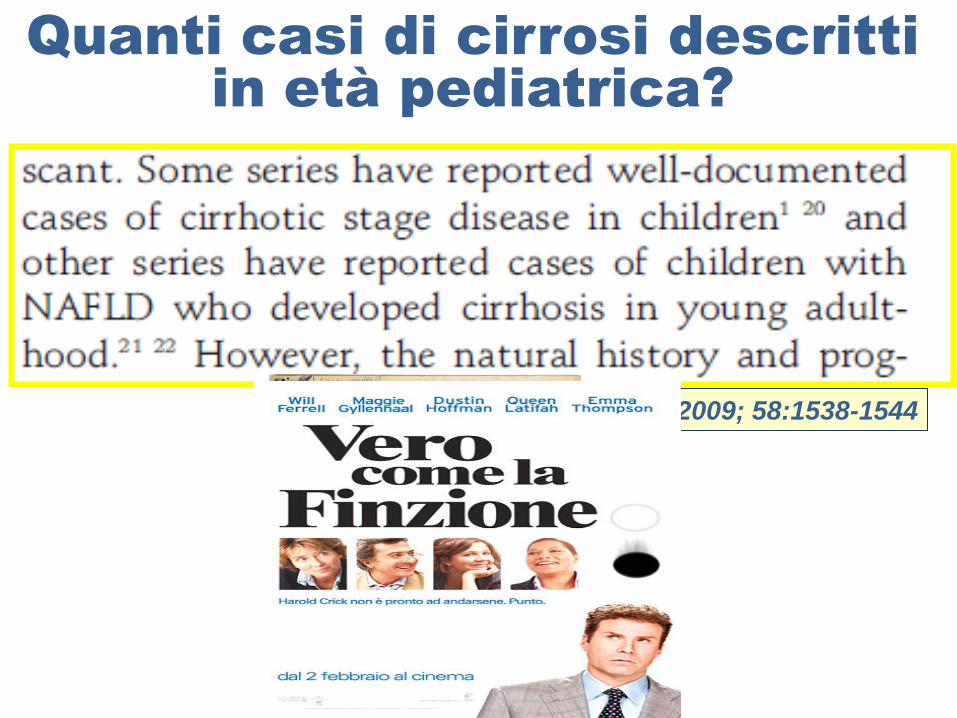
Quanti casi di cirrosi descritti
in età pediatrica?
Gut 2009; 58:1538-1544
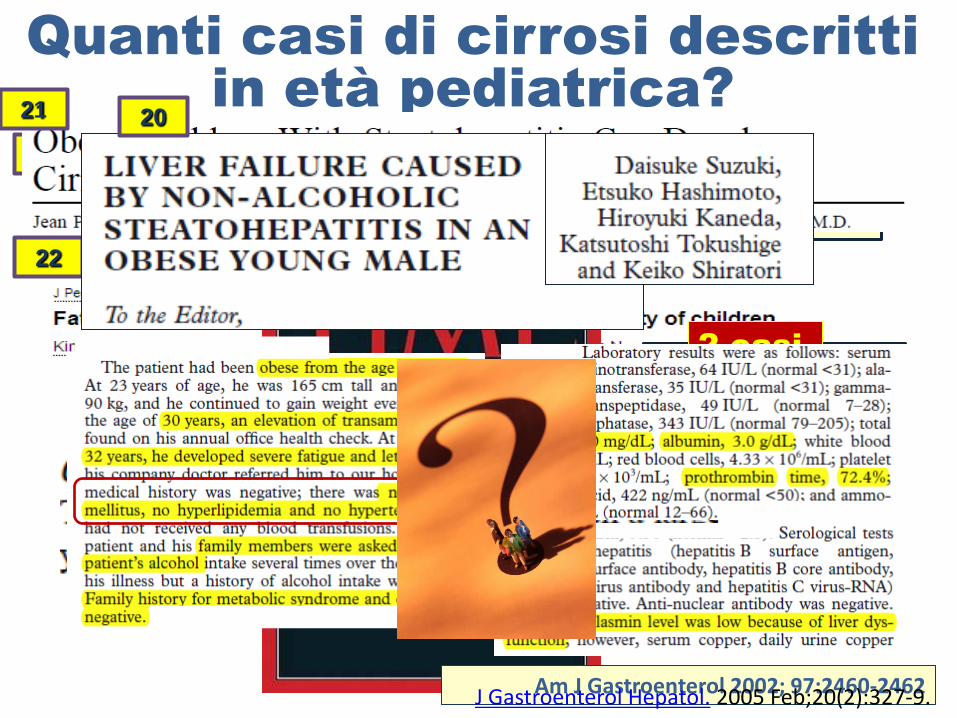
Quanti casi di cirrosi descritti
in età pediatrica?
1/43 steatosi: cirrosi
1
1/299 obesi: cirrosi
Am J Gastroenterol 2002; 97:2460-2462
21
2 casi
22
20
J Gastroenterol Hepatol. 2005 Feb;20(2):327-9.
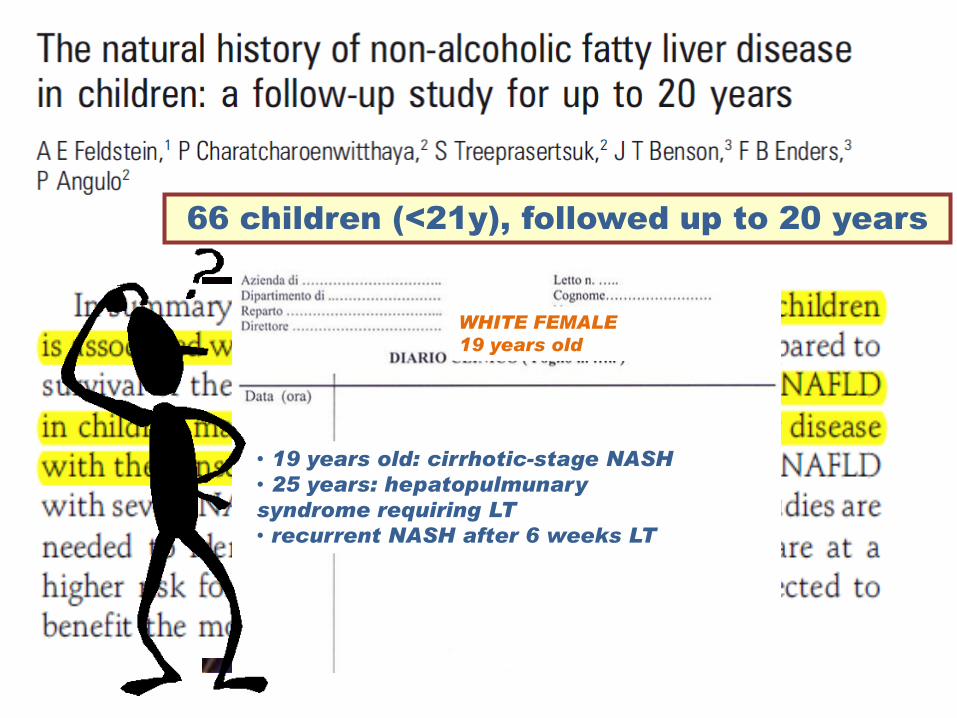
66 children (<21y), followed up to 20 years
• 11 years old: grade 3 varices
• recurrent variceal bleeding
• 20 years old: liver trasplantation
• recurrent NASH after 9 months LT
• 19 years old: cirrhotic-stage NASH
• 25 years: hepatopulmunary
syndrome requiring LT
• recurrent NASH after 6 weeks LT
HISPANIC FEMALE
11 years old
WHITE FEMALE
19 years old
RECURRENCE OF NASH AFTER LT IN CHILDREN
Liv Transpl 2005; 11:108-110
Pediatr Transplant 2007; 11:796-99
Hepatology 2004;39:909-914
Quanti casi di cirrosi descritti
in età pediatrica?
Gut 2009; 58:1538-1544
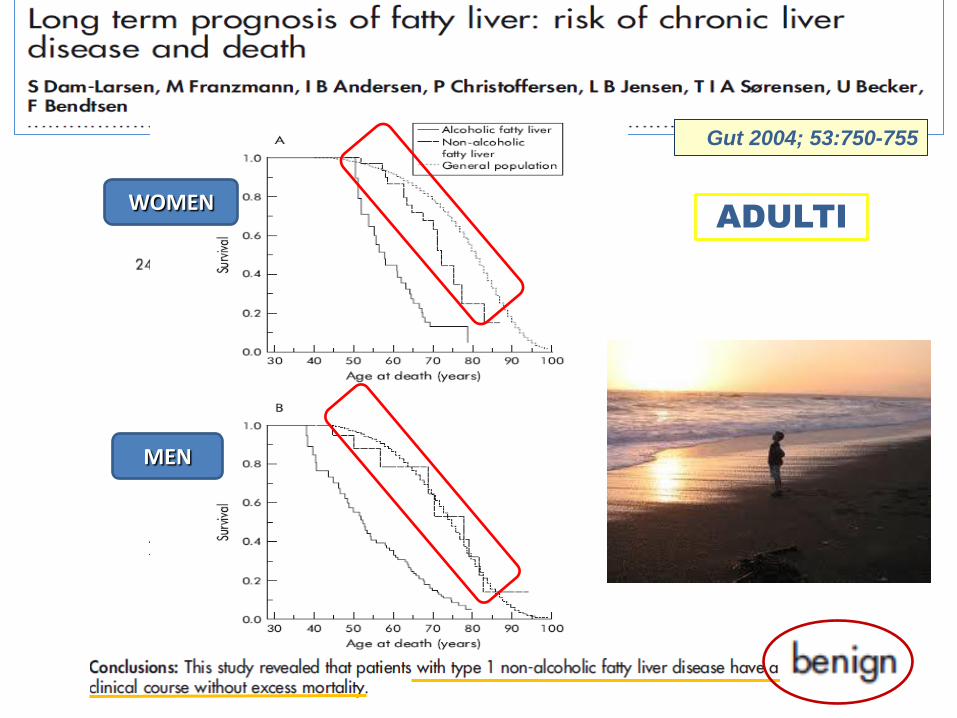
Gut 2004; 53:750-755
WOMEN
MEN
ADULTI
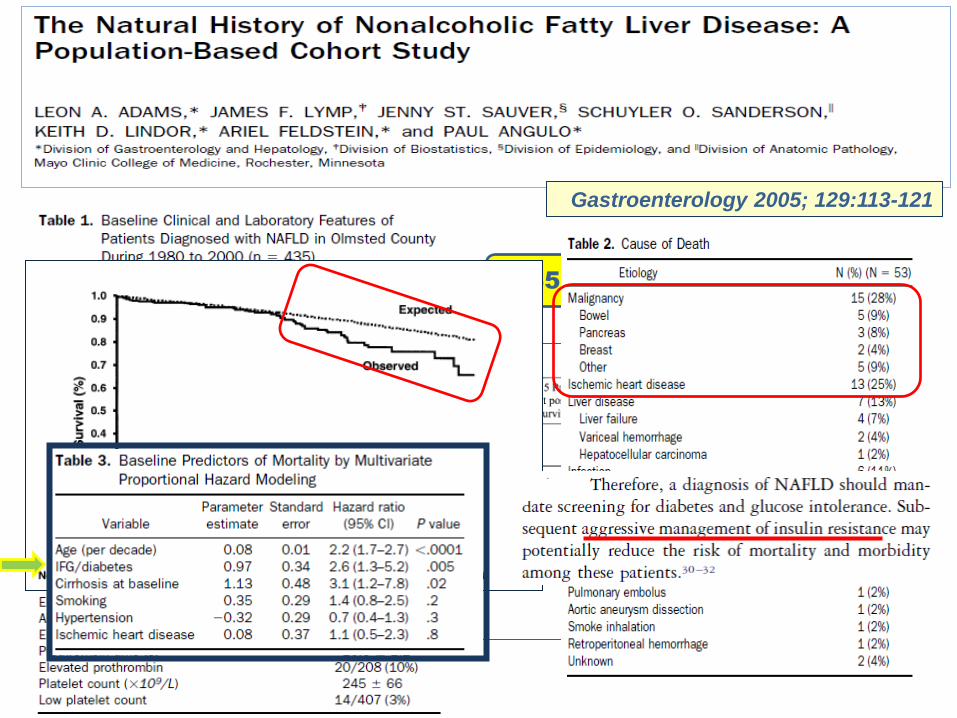
Gastroenterology 2005; 129:113-121
435 PZ
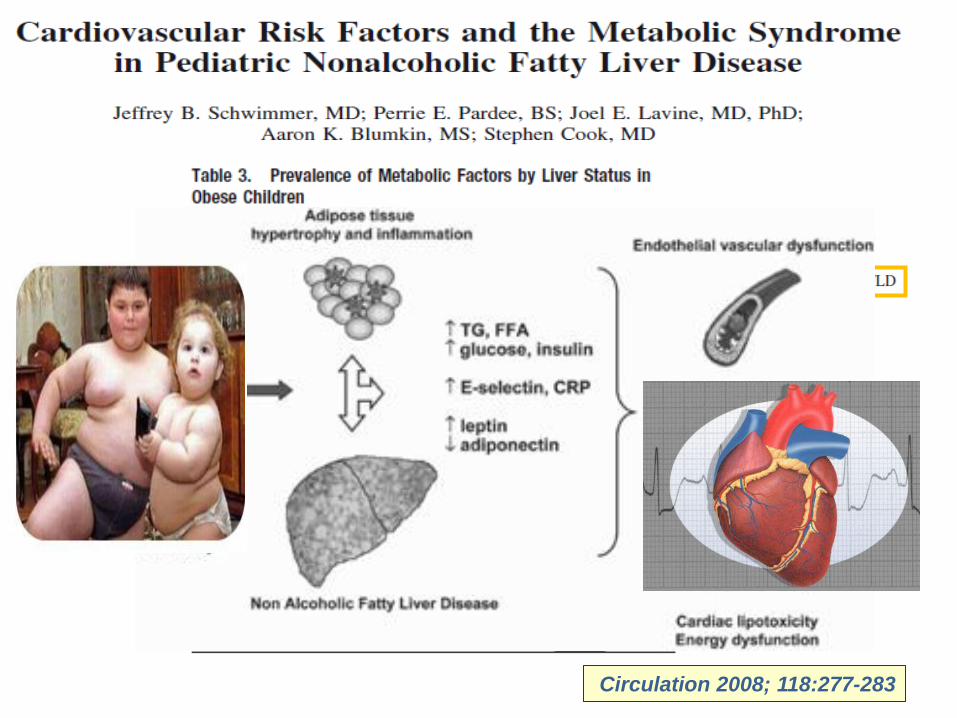
Circulation 2008; 118:277-283

Quanti sono i casi di NAFLD che
richiedono l’epatotrapianto ?
Liver Transpl. 2001 ;7:608-14
ADULTI
The percentage of patients undergoing a liver transplant for NASH increased from 1.2% in 2001 to 9.7% in 2009
Gastroenterology 2011;141(4):1249-1253
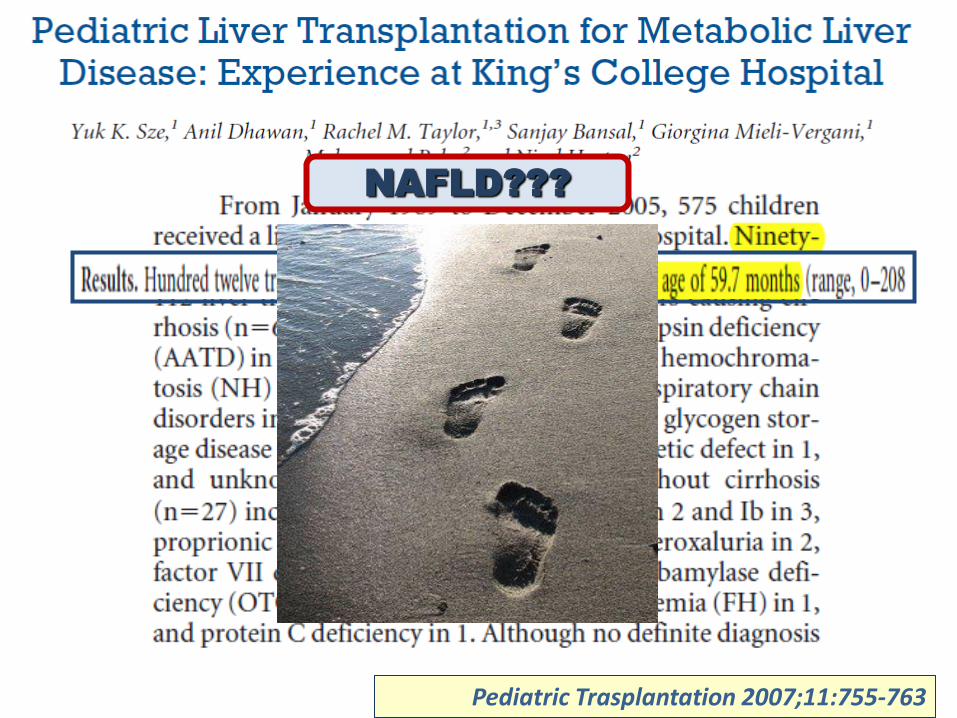
Pediatric Trasplantation 2007;11:755-763
NAFLD???
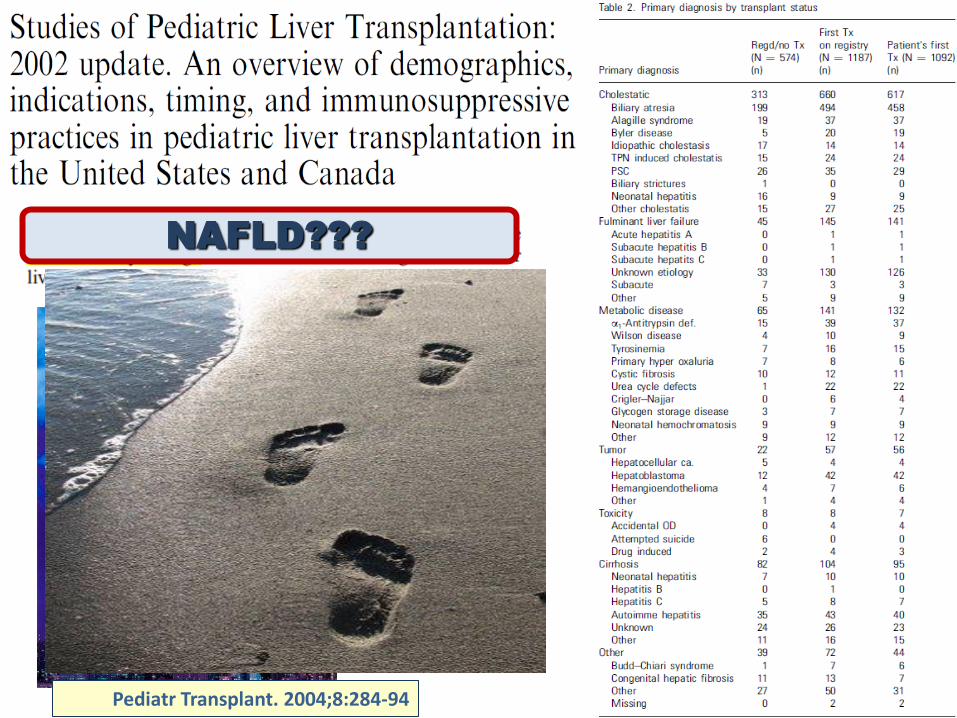
NAFLD???
Pediatr Transplant. 2004;8:284-94
TERAPIA della NAFLD?
Pediatric Diabetes 2009;10:1-4
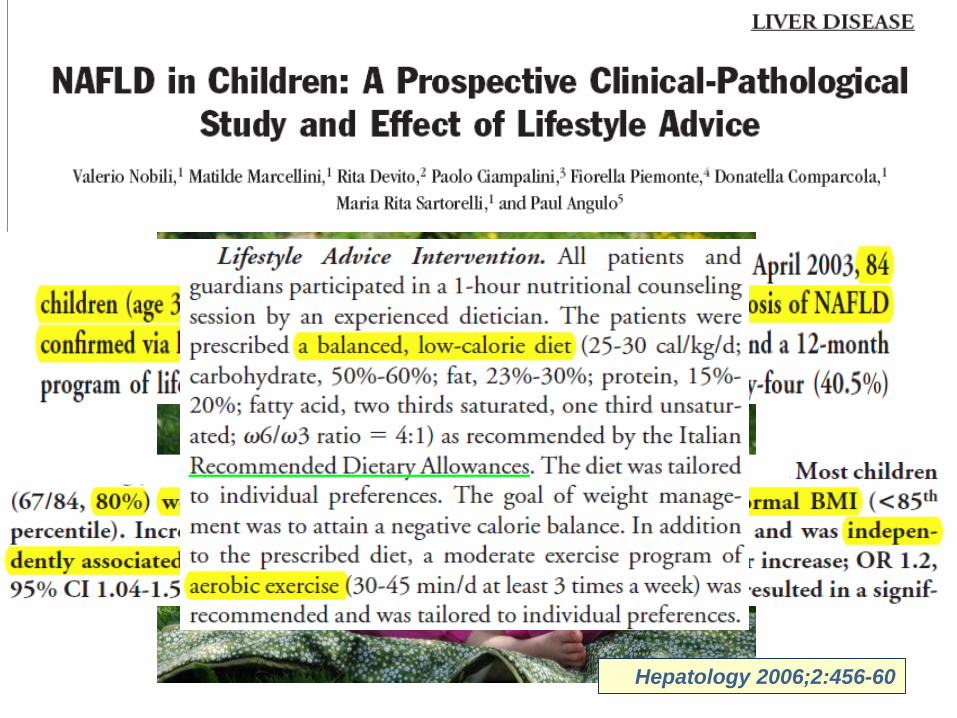
Hepatology 2006;2:456-60
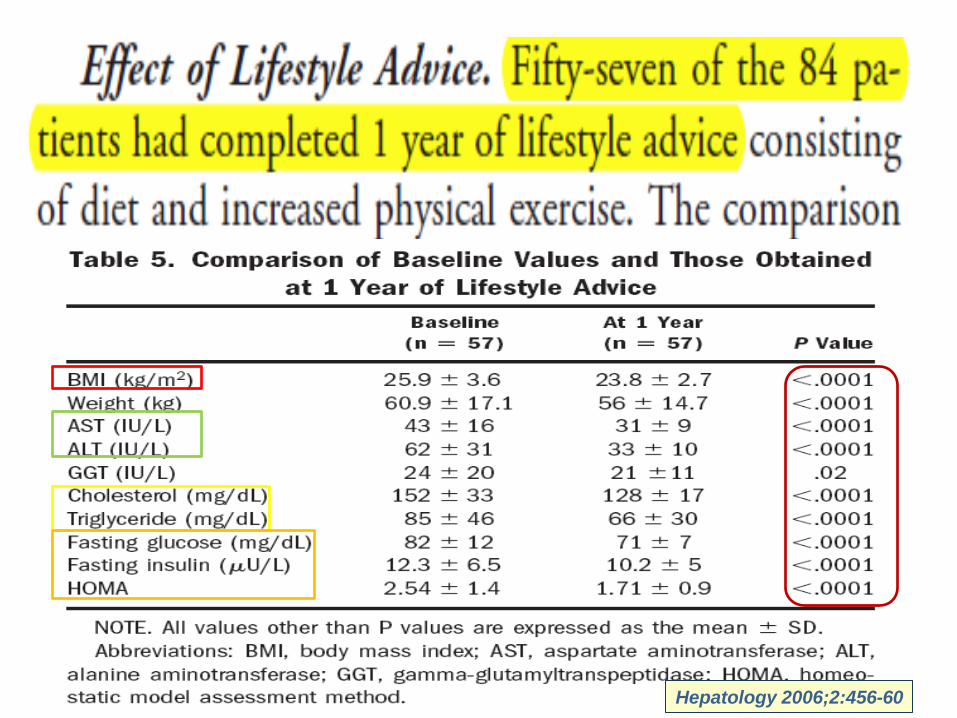
68%
Hepatology 2006;2:456-60
Quando il gatto non c’è….
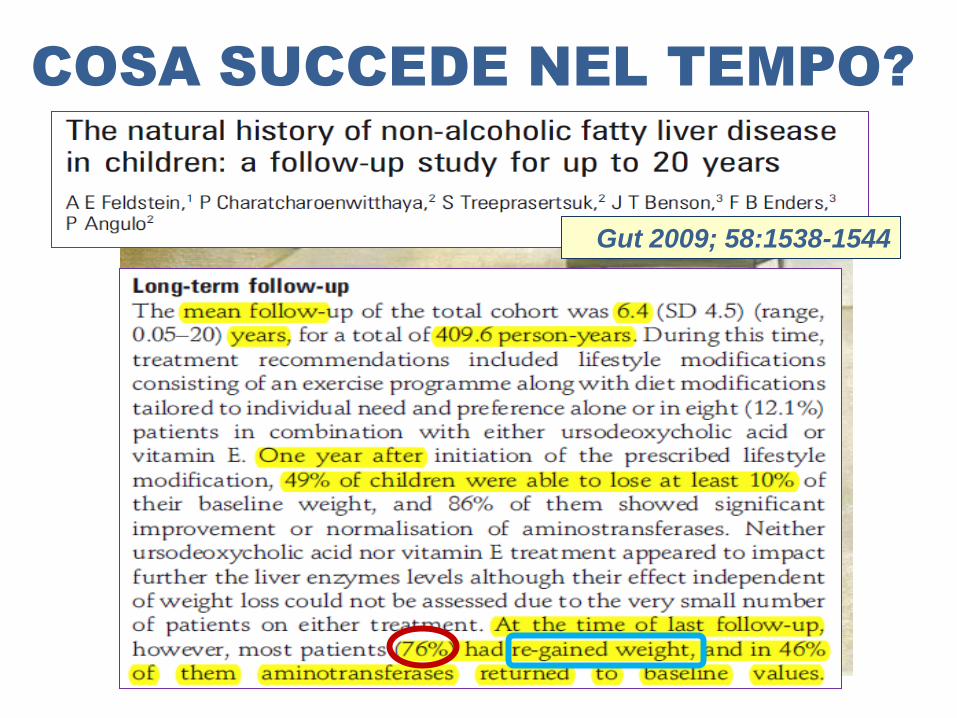
COSA SUCCEDE NEL TEMPO?
Gut 2009; 58:1538-1544
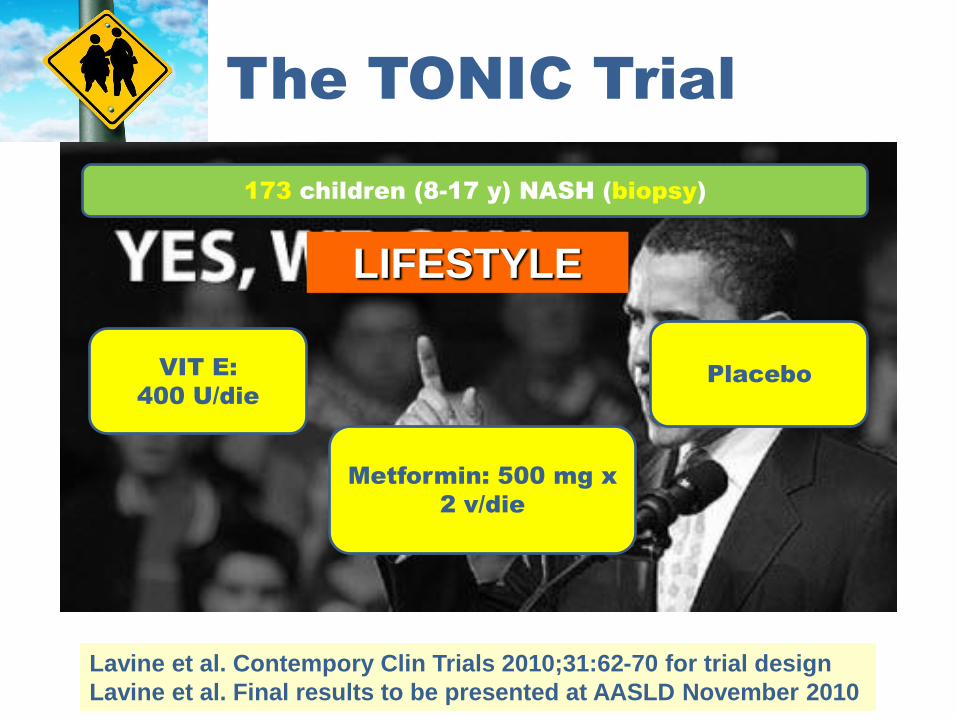
The TONIC Trial
Lavine et al. Contempory Clin Trials 2010;31:62-70 for trial design
Lavine et al. Final results to be presented at AASLD November 2010
173 children (8-17 y) NASH (biopsy)
VIT E:
400 U/die
Metformin: 500 mg x
2 v/die
Placebo
LIFESTYLE
Hepatology, 2010; 52:1274-1281
Sinusoidal Endothelial Dysfunction PrecedesInflammation and Fibrosis in a Model of NAFLD
Marcos Pasarın, Vincenzo La Mura, Jorge Gracia-Sancho, Hector Garcıa-Caldero, Aina Rodrıguez-
Vilarrupla, Juan Carlos Garcıa-Pagan, Jaime Bosch, Juan G. Abraldes*
Hepatic Hemodynamic Laboratory, Liver Unit, Hospital Clınic-IDIBAPS, CIBERrehd, University of Barcelona, Barcelona, Spain
Abst ract
Non-alcoholic fatty liver disease (NAFLD) is the hepatic manifestation of the metabolic syndrome. Most morbidity associatedwith the metabolic syndrome is related to vascular complications, in which endothelial dysfunction is a major pathogenicfactor. However, whether NAFLD is associated with endothelial dysfunction within the hepatic vasculature is unknown. Theaims of this study were to explore, in a model of diet-induced overweight that expresses most features of the metabolicsyndrome, whether early NAFLD is associated with liver endothelial dysfunction. Wistar Kyoto rats were fed a cafeteria diet(CafD; 65% of fat, mostly saturated) or a control diet (CD) for 1 month. CafD rats developed features of the metabolicsyndrome (overweight, arterial hypertension, hypertryglyceridemia, hyperglucemia and insulin resistance) and liver steatosiswithout inflammation or fibrosis. CafD rats had a significantly higher in vivo hepatic vascular resistance than CD. In liverperfusion livers from CafD rats had an increased portal perfusion pressure and decreased endothelium-dependentvasodilation. This was associated with a decreased Akt-dependent eNOSphosphorylation and NOSactivity. In summary, wedemonstrate in a rat model of the metabolic syndrome that shows features of NAFLD, that liver endothelial dysfunctionoccurs before the development of fibrosis or inflammation.
Citat ion: Pasarın M, La Mura V, Gracia-Sancho J, Garcıa-Caldero H, Rodrıguez-Vilarrupla A, et al. (2012) Sinusoidal Endothelial Dysfunction Precedes Inflammationand Fibrosis in a Model of NAFLD. PLoS ONE 7(4): e32785. doi:10.1371/journal.pone.0032785
Editor: Massimo Federici, University of Tor Vergata, Italy
Received June 28, 2011; Accepted February 3, 2012; Published April 3, 2012
Copyright : ß 2012 Pasarın et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was supported by grants from the Instituto de Salud Carlos III (FIS05/0519 and FIS08/0193 to Dr. Abraldes and Dr. Pasarın 09/01261 to Dr.Bosch), and co-financed by FEDER funds (EU, ‘‘Una manera de hacer Europa‘‘). Part of this work was carried out at the Esther Koplowitz Centre, Barcelona.Ciberehd is funded by Instituto de Salud Carlos III. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of themanuscript.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Int roduct ion
The metabolic syndrome is defined as a combination of
abnormalities including central obesity, hypertriglyceridemia,
low levels of HDL cholesterol, hypertension and hyperglycemia
[1]. Insulin resistance (IR) is thought to be the pathophysiological
hallmark of the syndrome [2,3]. Non-alcoholic fatty liver disease
(NAFLD) is the hepatic expression of the metabolic syndrome and
has an increasing prevalence in the western population [4]. The
spectrum of NAFLD lesions is wide, and goes from simple
steatosis, non-alcoholic steatotohepatitis (inflammation, features of
hepatocyte injury with or without fibrosis), to overt cirrhosis [5].
The mechanisms that account for disease progression in NAFLD
are still poorly understood.
Most complications leading to morbidity in patients with the
metabolic syndrome are of vascular origin [6]. One of the factors
contributing to vascular disease in this setting is the presence of
endothelial dysfunction, with decreased nitric oxide (NO)
production [7], which has been consistently observed before
cardiovascular events occur, and even before any pathological
abnormalities in the vascular tree can be demonstrated [8]. This
suggests that endothelial dysfunction is an early pathogenic event
in the course of the vascular complications that occur in these
patients. In keeping with this concept, correction of endothelial
dysfunction is associated with an improvement in the rates of
vascular eventsand, therefore, it isconsidered a useful therapeutic
target in thissyndrome [9,10]. Interestingly, patientswith NAFLD
exhibit systemic endothelial dysfunction and a increased cardio-
vascular risk [11].
The liver sinusoidal endothelium is a very specialized and
phenotypically differentiated endothelium, being its major speci-
ficities the presence of fenestrae and the absence of basal
membrane [12]. Among other functions, an adequately function-
ing sinusoidal endothelium maintains an anti-inflammatory, anti-
thrombotic and anti-fibrotic milieu within the liver parenchyma
[13–15].
Some recent data have shown the presence of microvascular
abnormalities in models of fatty liver, characterized by the
presence of reduced sinusoidal perfusion [16] and structurally
abnormal sinusoidsdue to lipid accumulation in parenchymal cells
and to collagen deposition in thespace of Disse [17]. However, the
presence of liver endothelial dysfunction has not been specifically
investigated. In addition, whether endothelial dysfunction might
occur earlier than other featuresof advanced NAFLD (as it occurs
in the peripheral circulation where endothelial dysfunction
precedes the development of arteriosclerosis) is largely unknown.
The aims of this study were to characterize the changes in liver
histology and liver microcirculatory function in a model of diet-
induced obesity that expresses most features of the metabolic
syndrome.
PLoS ONE | www.plosone.org 1 April 2012 | Volume 7 | Issue 4 | e32785
Sinusoidal Endothelial Dysfunction PrecedesInflammation and Fibrosis in a Model of NAFLD
Marcos Pasarın, Vincenzo La Mura, Jorge Gracia-Sancho, Hector Garcıa-Caldero, Aina Rodrıguez-
Vilarrupla, Juan Carlos Garcıa-Pagan, Jaime Bosch, Juan G. Abraldes*
Hepatic Hemodynamic Laboratory, Liver Unit, Hospital Clınic-IDIBAPS, CIBERrehd, University of Barcelona, Barcelona, Spain
Abstract
Non-alcoholic fatty liver disease (NAFLD) isthe hepatic manifestation of the metabolic syndrome. Most morbidity associatedwith the metabolic syndrome is related to vascular complications, in which endothelial dysfunction is a major pathogenicfactor. However, whether NAFLD is associated with endothelial dysfunction within the hepatic vasculature is unknown. Theaims of this study were to explore, in a model of diet-induced overweight that expresses most features of the metabolicsyndrome, whether early NAFLD is associated with liver endothelial dysfunction. Wistar Kyoto rats were fed a cafeteria diet(CafD; 65% of fat, mostly saturated) or a control diet (CD) for 1 month. CafD rats developed features of the metabolicsyndrome (overweight, arterial hypertension, hypertryglyceridemia, hyperglucemia and insulin resistance) and liver steatosiswithout inflammation or fibrosis. CafD rats had a significantly higher in vivo hepatic vascular resistance than CD. In liverperfusion livers from CafD rats had an increased portal perfusion pressure and decreased endothelium-dependentvasodilation. This wasassociated with a decreased Akt-dependent eNOSphosphorylation and NOSactivity. In summary, wedemonstrate in a rat model of the metabolic syndrome that shows features of NAFLD, that liver endothelial dysfunctionoccurs before the development of fibrosis or inflammation.
Citation: Pasarın M, La Mura V, Gracia-Sancho J,Garcıa-Caldero H,Rodrıguez-Vilarrupla A, et al. (2012) Sinusoidal Endothelial Dysfunction Precedes Inflammationand Fibrosis in a Model of NAFLD. PLoSONE 7(4): e32785. doi:10.1371/journal.pone.0032785
Editor: Massimo Federici, University of Tor Vergata, Italy
Received June 28, 2011; Accepted February 3, 2012; Published April 3, 2012
Copyright: ß 2012 Pasarın et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was supported by grants from the Instituto de Salud Carlos III (FIS05/0519 and FIS08/0193 to Dr. Abraldes and Dr. Pasarın 09/01261 to Dr.Bosch), and co-financed by FEDER funds (EU, ‘‘Una manera de hacer Europa‘‘). Part of this work was carried out at the Esther Koplowitz Centre, Barcelona.Ciberehd is funded by Instituto de Salud Carlos III. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of themanuscript.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduct ion
The metabolic syndrome is defined as a combination of
abnormalities including central obesity, hypertriglyceridemia,
low levels of HDL cholesterol, hypertension and hyperglycemia
[1]. Insulin resistance (IR) is thought to be the pathophysiological
hallmark of the syndrome [2,3]. Non-alcoholic fatty liver disease
(NAFLD) isthe hepatic expression of the metabolic syndrome and
has an increasing prevalence in the western population [4]. The
spectrum of NAFLD lesions is wide, and goes from simple
steatosis, non-alcoholic steatotohepatitis (inflammation, features of
hepatocyte injury with or without fibrosis), to overt cirrhosis [5].
The mechanisms that account for disease progression in NAFLD
are still poorly understood.
Most complications leading to morbidity in patients with the
metabolic syndrome are of vascular origin [6]. One of the factors
contributing to vascular disease in this setting is the presence of
endothelial dysfunction, with decreased nitric oxide (NO)
production [7], which has been consistently observed before
cardiovascular events occur, and even before any pathological
abnormalities in the vascular tree can be demonstrated [8]. This
suggests that endothelial dysfunction is an early pathogenic event
in the course of the vascular complications that occur in these
patients. In keeping with this concept, correction of endothelial
dysfunction is associated with an improvement in the rates of
vascular eventsand, therefore, it isconsidered a useful therapeutic
target in thissyndrome [9,10]. Interestingly, patientswith NAFLD
exhibit systemic endothelial dysfunction and a increased cardio-
vascular risk [11].
The liver sinusoidal endothelium is a very specialized and
phenotypically differentiated endothelium, being its major speci-
ficities the presence of fenestrae and the absence of basal
membrane [12]. Among other functions, an adequately function-
ing sinusoidal endothelium maintains an anti-inflammatory, anti-
thrombotic and anti-fibrotic milieu within the liver parenchyma
[13–15].
Some recent data have shown the presence of microvascular
abnormalities in models of fatty liver, characterized by the
presence of reduced sinusoidal perfusion [16] and structurally
abnormal sinusoidsdueto lipid accumulation in parenchymal cells
and to collagen deposition in thespaceof Disse [17]. However, the
presence of liver endothelial dysfunction has not been specifically
investigated. In addition, whether endothelial dysfunction might
occur earlier than other featuresof advanced NAFLD (asit occurs
in the peripheral circulation where endothelial dysfunction
precedes the development of arteriosclerosis) is largely unknown.
The aimsof thisstudy were to characterize the changes in liver
histology and liver microcirculatory function in a model of diet-
induced obesity that expresses most features of the metabolic
syndrome.
PLoS ONE | www.plosone.org 1 April 2012 | Volume 7 | Issue 4 | e32785
Sinusoidal Endothelial Dysfunction PrecedesInflammation and Fibrosis in a Model of NAFLD
Marcos Pasarın, Vincenzo La Mura, Jorge Gracia-Sancho, Hector Garcıa-Caldero, Aina Rodrıguez-
Vilarrupla, Juan Carlos Garcıa-Pagan, Jaime Bosch, Juan G. Abraldes*
Hepatic Hemodynamic Laboratory, Liver Unit, Hospital Clınic-IDIBAPS, CIBERrehd, University of Barcelona, Barcelona, Spain
Abst ract
Non-alcoholic fatty liver disease (NAFLD) is the hepatic manifestation of the metabolic syndrome. Most morbidity associatedwith the metabolic syndrome is related to vascular complications, in which endothelial dysfunction is a major pathogenicfactor. However, whether NAFLD isassociated with endothelial dysfunction within the hepatic vasculature is unknown. Theaims of this study were to explore, in a model of diet-induced overweight that expresses most features of the metabolicsyndrome, whether early NAFLD is associated with liver endothelial dysfunction. Wistar Kyoto rats were fed a cafeteria diet(CafD; 65% of fat, mostly saturated) or a control diet (CD) for 1 month. CafD rats developed features of the metabolicsyndrome (overweight, arterial hypertension, hypertryglyceridemia, hyperglucemia and insulin resistance) and liver steatosiswithout inflammation or fibrosis. CafD rats had a significantly higher in vivo hepatic vascular resistance than CD. In liverperfusion livers from CafD rats had an increased portal perfusion pressure and decreased endothelium-dependentvasodilation. This was associated with a decreased Akt-dependent eNOSphosphorylation and NOSactivity. In summary, wedemonstrate in a rat model of the metabolic syndrome that shows features of NAFLD, that liver endothelial dysfunctionoccurs before the development of fibrosis or inflammation.
Citation: Pasarın M, La Mura V, Gracia-Sancho J,Garcıa-Caldero H,Rodrıguez-Vilarrupla A, et al. (2012) Sinusoidal Endothelial Dysfunction Precedes Inflammationand Fibrosis in a Model of NAFLD. PLoSONE 7(4): e32785. doi:10.1371/journal.pone.0032785
Editor: Massimo Federici, University of Tor Vergata, Italy
Received June 28, 2011; Accepted February 3, 2012; Published April 3, 2012
Copyright: ß 2012 Pasarın et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was supported by grants from the Instituto de Salud Carlos III (FIS05/0519 and FIS08/0193 to Dr. Abraldes and Dr. Pasarın 09/01261 to Dr.Bosch), and co-financed by FEDER funds (EU, ‘‘Una manera de hacer Europa‘‘). Part of this work was carried out at the Esther Koplowitz Centre, Barcelona.Ciberehd is funded by Instituto de Salud Carlos III. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of themanuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduct ion
The metabolic syndrome is defined as a combination of
abnormalities including central obesity, hypertriglyceridemia,
low levels of HDL cholesterol, hypertension and hyperglycemia
[1]. Insulin resistance (IR) is thought to be the pathophysiological
hallmark of the syndrome [2,3]. Non-alcoholic fatty liver disease
(NAFLD) isthe hepatic expression of the metabolic syndrome and
has an increasing prevalence in the western population [4]. The
spectrum of NAFLD lesions is wide, and goes from simple
steatosis, non-alcoholic steatotohepatitis (inflammation, featuresof
hepatocyte injury with or without fibrosis), to overt cirrhosis [5].
The mechanisms that account for disease progression in NAFLD
are still poorly understood.
Most complications leading to morbidity in patients with the
metabolic syndrome are of vascular origin [6]. One of the factors
contributing to vascular disease in this setting is the presence of
endothelial dysfunction, with decreased nitric oxide (NO)
production [7], which has been consistently observed before
cardiovascular events occur, and even before any pathological
abnormalities in the vascular tree can be demonstrated [8]. This
suggests that endothelial dysfunction is an early pathogenic event
in the course of the vascular complications that occur in these
patients. In keeping with this concept, correction of endothelial
dysfunction is associated with an improvement in the rates of
vascular eventsand, therefore, it isconsidered a useful therapeutic
target in thissyndrome [9,10]. Interestingly, patientswith NAFLD
exhibit systemic endothelial dysfunction and a increased cardio-
vascular risk [11].
The liver sinusoidal endothelium is a very specialized and
phenotypically differentiated endothelium, being its major speci-
ficities the presence of fenestrae and the absence of basal
membrane [12]. Among other functions, an adequately function-
ing sinusoidal endothelium maintains an anti-inflammatory, anti-
thrombotic and anti-fibrotic milieu within the liver parenchyma
[13–15].
Some recent data have shown the presence of microvascular
abnormalities in models of fatty liver, characterized by the
presence of reduced sinusoidal perfusion [16] and structurally
abnormal sinusoidsdueto lipid accumulation in parenchymal cells
and to collagen deposition in thespaceof Disse [17]. However, the
presence of liver endothelial dysfunction has not been specifically
investigated. In addition, whether endothelial dysfunction might
occur earlier than other featuresof advanced NAFLD (asit occurs
in the peripheral circulation where endothelial dysfunction
precedes the development of arteriosclerosis) is largely unknown.
The aimsof thisstudy were to characterize the changes in liver
histology and liver microcirculatory function in a model of diet-
induced obesity that expresses most features of the metabolic
syndrome.
PLoSONE | www.plosone.org 1 April 2012 | Volume 7 | Issue 4 | e32785
Journal of Nutritional Biochemistry 2011; in press
Ho smesso di fumare. Vivrò una settimana di più e in quella settimana pioverà a dirotto!
Woody Allen

















